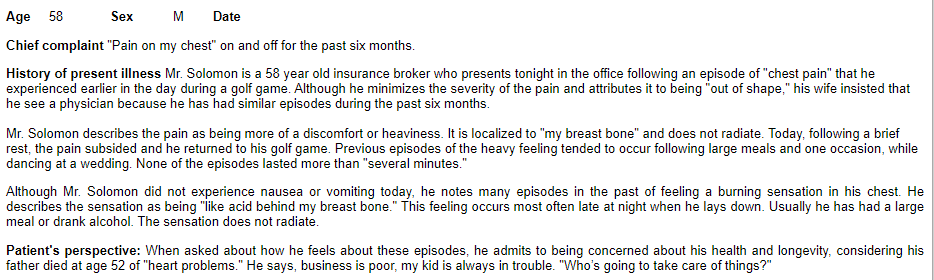
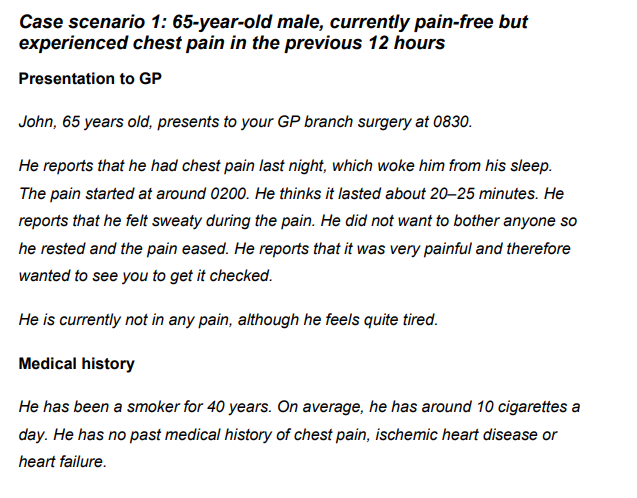
This vignette describes chronic (stable) angina pretty well - and it helps me understand the clinical profile of the persons belonging to this category
http://www.meddean.luc.edu/lumen/meded/mech/cases/case1/Caseqa_f.htm
| OHDSI Home | Forums | Wiki | Github |

This vignette describes chronic (stable) angina pretty well - and it helps me understand the clinical profile of the persons belonging to this category
http://www.meddean.luc.edu/lumen/meded/mech/cases/case1/Caseqa_f.htm
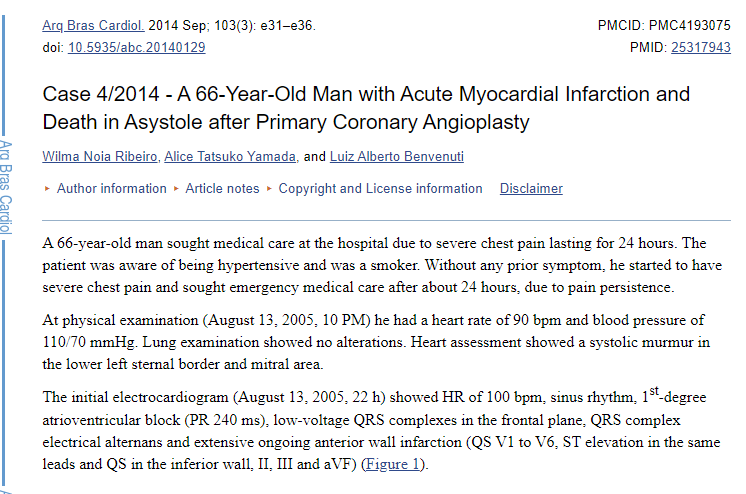
This appears to be a case of myocardial infarction (most probably a STEMI but the presentation appears to be late)
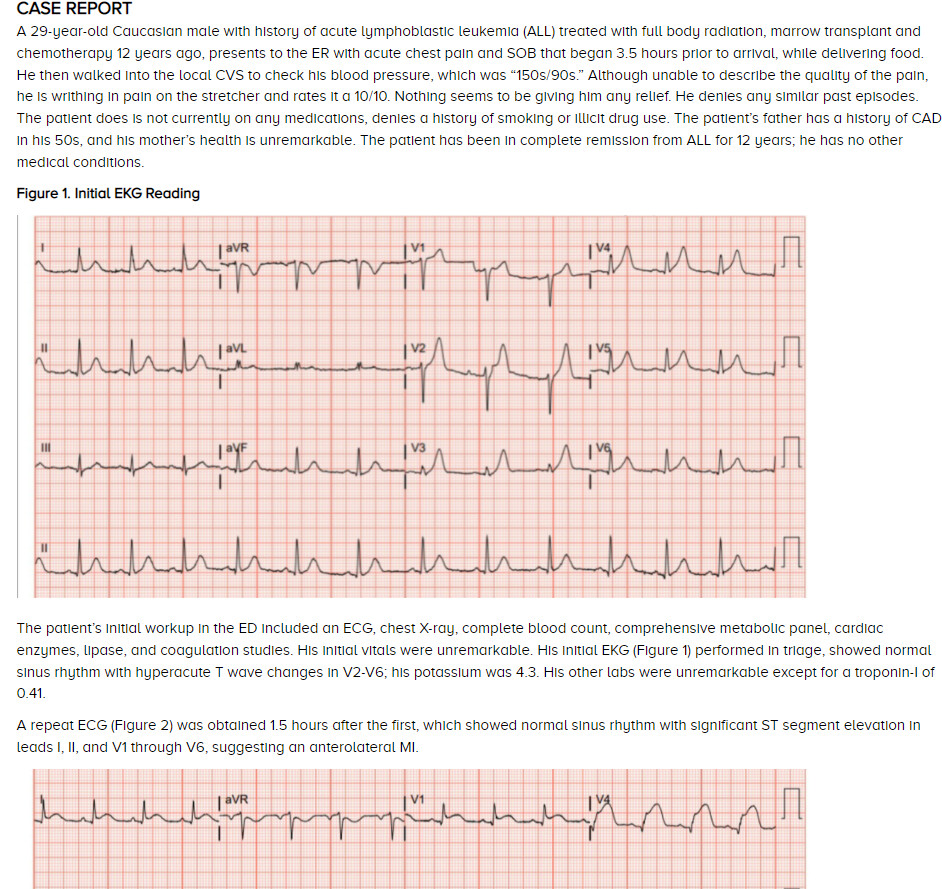
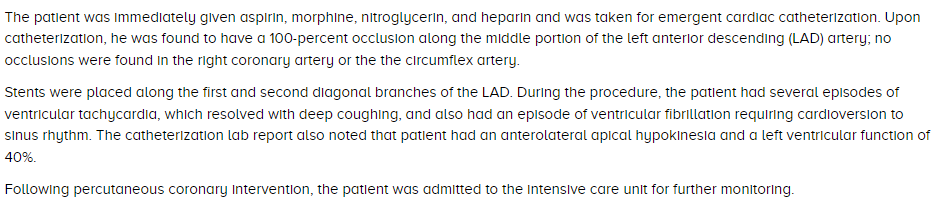
Here is a case report - where a person evolved into STEMI while in direct observation (with serial EKG)
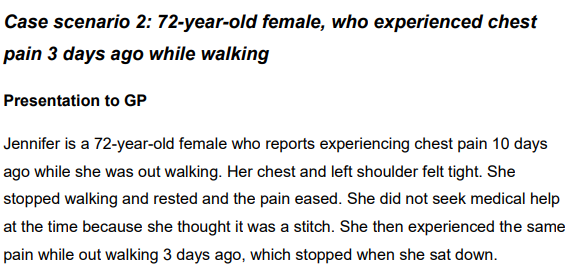
A case report - where the chest pain has already resolved
https://www.nice.org.uk/guidance/cg126/resources/chest-pain-algorithm-clinical-case-scenarios-pdf-243970669
And another (again not MI)
https://www.nice.org.uk/guidance/cg126/resources/chest-pain-algorithm-clinical-case-scenarios-pdf-243970669
Next step literature review - there appears to be many publications that have evaluated the validity of cohort definitions (or atleast code sets) in observational data. From common attributes that i was able to find
Thank you again Ms. Gayle Murray for leading the effort on this systematic literature search. Her contribution is also described here
Some key materials are
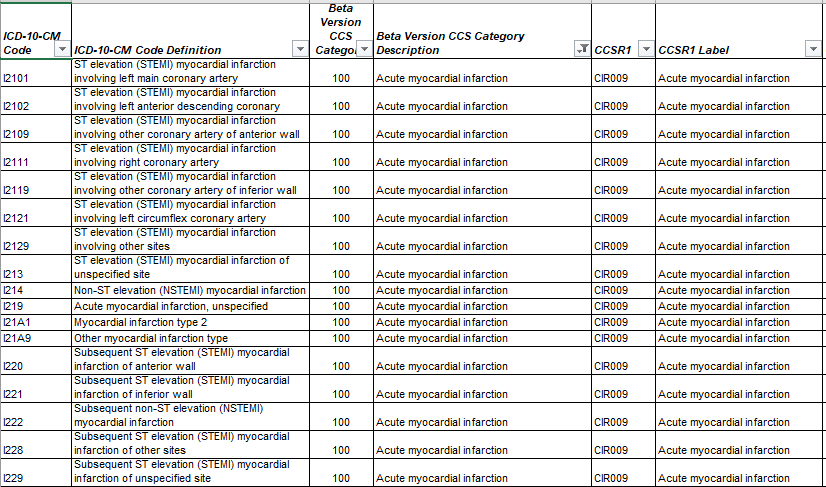
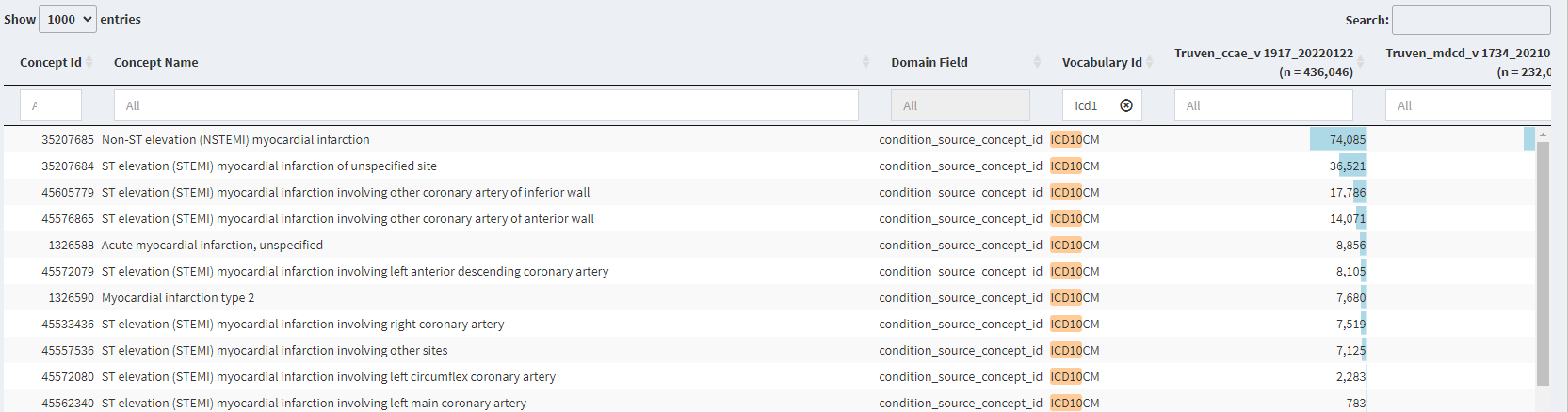
Based on the literature search - the codes used by various literature sources were collated (presenting only ICD and DRG for simplicity)
| Code | Vocabulary |
|---|---|
| 121 | DRG |
| 122 | DRG |
| 123 | DRG |
| I21 | ICD10 |
| I21.x | ICD10 |
| I22 | ICD10 |
| I23 | ICD10 |
| I21.x | ICD-10-CM |
| I22.x | ICD-10-CM |
| 410.0 | ICD9 |
| 410.01 | ICD9 |
| 410.02 | ICD9 |
| 410.1 | ICD9 |
| 410.11 | ICD9 |
| 410.12 | ICD9 |
| 410.2 | ICD9 |
| 410.21 | ICD9 |
| 410.22 | ICD9 |
| 410.3 | ICD9 |
| 410.31 | ICD9 |
| 410.32 | ICD9 |
| 410.4 | ICD9 |
| 410.41 | ICD9 |
| 410.42 | ICD9 |
| 410.5 | ICD9 |
| 410.51 | ICD9 |
| 410.52 | ICD9 |
| 410.6 | ICD9 |
| 410.61 | ICD9 |
| 410.62 | ICD9 |
| 410.7 | ICD9 |
| 410.71 | ICD9 |
| 410.72 | ICD9 |
| 410.7x | ICD9 |
| 410.8 | ICD9 |
| 410.81 | ICD9 |
| 410.82 | ICD9 |
| 410.9 | ICD9 |
| 410.91 | ICD9 |
| 410.91; | ICD9 |
| 410.92 | ICD9 |
| 410.x | ICD9 |
| 410.x0 | ICD9 |
| 410.x1 | ICD9 |
| 410.xx | ICD9 |
| 410 | ICD-9 |
| 410 | ICD9CM |
| 410.x | ICD9CM |
| 410.X0 | ICD9CM |
| 410.X1 | ICD9CM |
These lists of ICD-9 and 10 codes are very similar to those I’ve used to identify acute myocardial infarction in studies I’ve worked on. However, when our goal has been to identify an actual AMI event date, we don’t include codes for old MI (ICD-9 412 and ICD-10 I25.2), or any codes indicating a “subsequent episode of care”, such as 410.x2 (where ‘x’ can be 0 through 9).
Agreed, @ershanno. I know in past OHDSI trainings (and in the cohort definition in Atlas Phenotype), we’ve simply excluded old MI from the MI standard concept, but it does look like concept 45766114 (Subsequent ST segment elevation myocardial infarction) could be a candidate for exclusion as well. I am trying to see if this concept truly acts a “subsequent” event in our data.
The ICD9CM range for old subsequent MIs (410.x2) do not seem to map to anything about the event being subsequent. Perhaps a mapping fix is needed?
So @Ajit_Londhe @ershanno what do you think of the clinical description written here
I agree with you the old MI does not fit well here - do you think we need to clarify that in our clinical description?
I know it’s a little off topic but I think this is where your use case maters. If you need to know that today is the day that you first had a heart attack this is very different from knowing if you have had an AMI or CAD or UA in the past for trial inclusion or covariate adjustment. We validated and fairly easily do you meet a clinical condition for outreach for enrollment in a clinical trial: Validation of a claims-based algorithm identifying eligible study subjects in the ADAPTABLE pragmatic clinical trial
A dental (they make me smile!) note indicating past medical history and medication reconciliation is enough to aid in confirmation of trial eligibility. Versus I need to know that today is the day some period post exposure to a COX-2 inhibitor that you first had an AMI.
Our clinical descriptions may change across research settings necessitating alternate phenotypes.
Absolutely - that why we want make writing of clinical description upfront a best practice.
So i think we agree - every cohort definition should accompany a clinical description that is based on the use case.
Just built the cohorts and am executing cohort diagnostics - lets review results tomorrow
I am anxious to learn from Cohort Diagnostics - can we truly differentiate between STEMI/NSTEMI/UA/Chronic Angina. In previous OHDSI work - i believe we have not differentiated between them.
@Ajit_Londhe and @ershanno do you have any additional insight on subsequent MI codes. From a pure semantic meaning - this would still be MI but
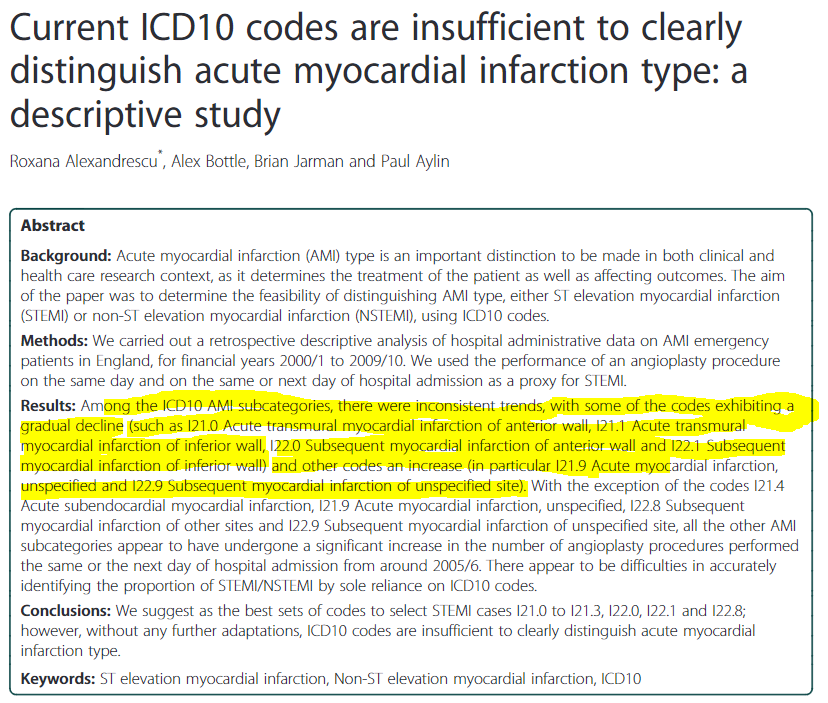
For example - i found this previous commentary on this topic Current ICD10 codes are insufficient to clearly distinguish acute myocardial infarction type: a descriptive study - PubMed
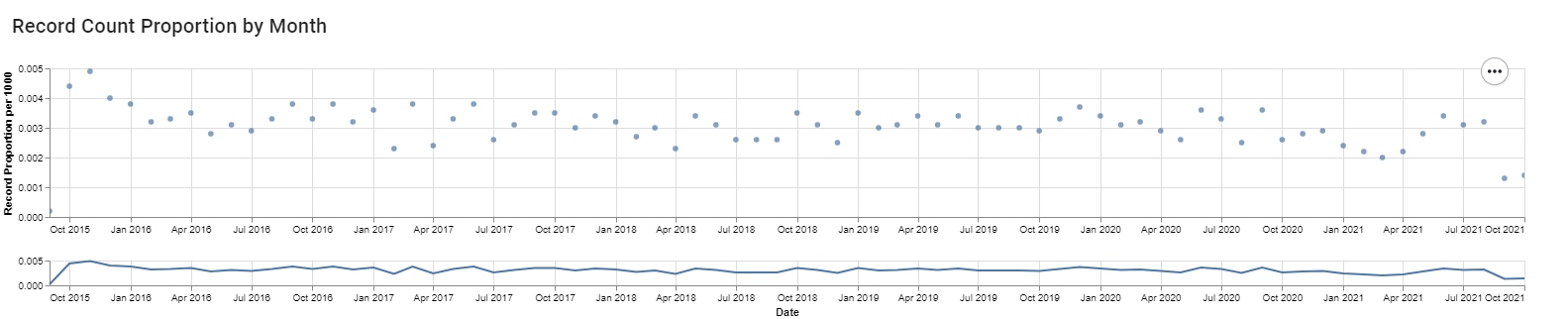
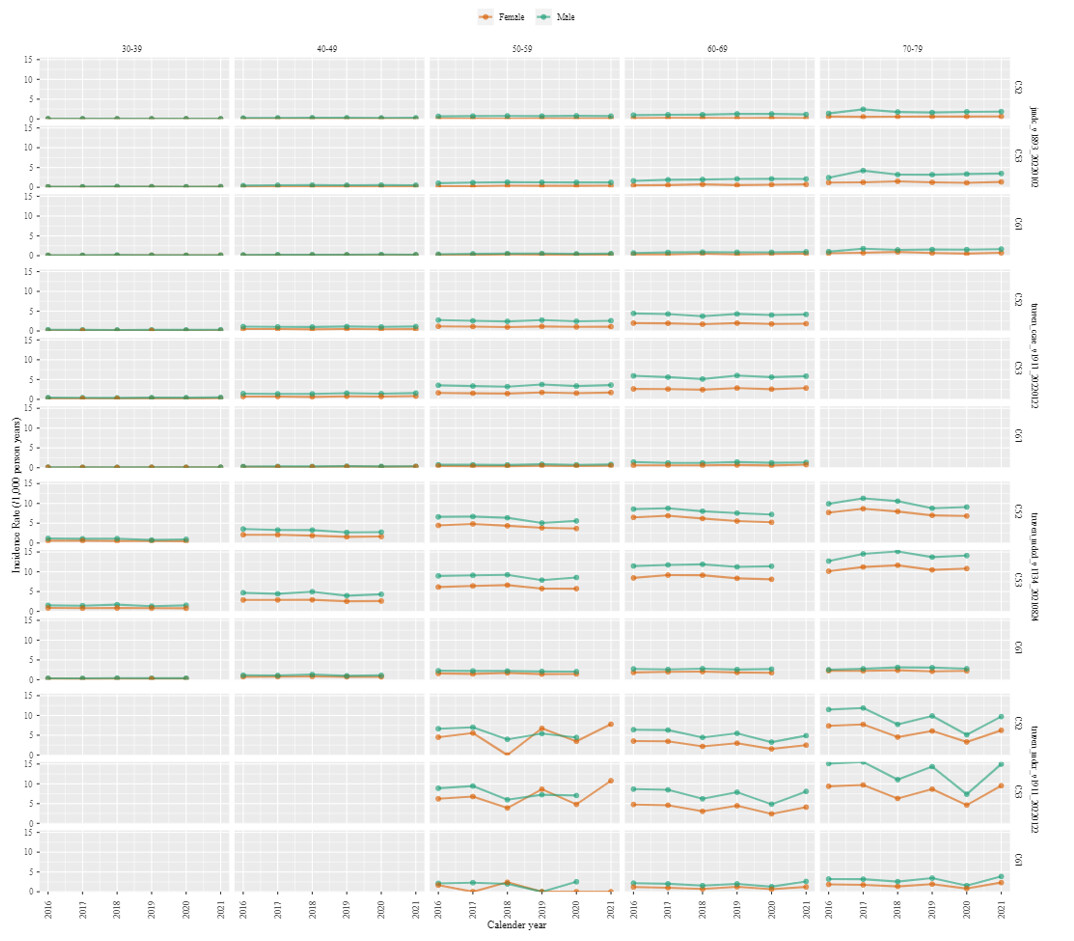
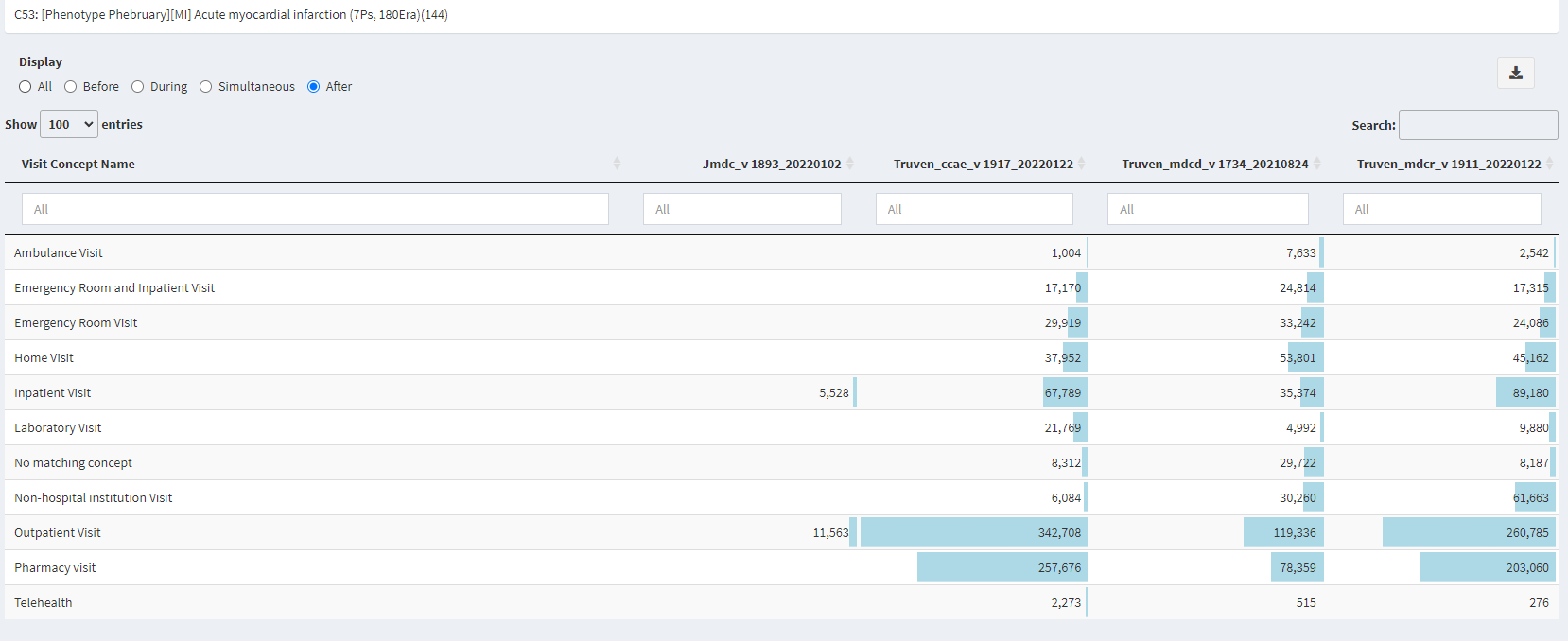
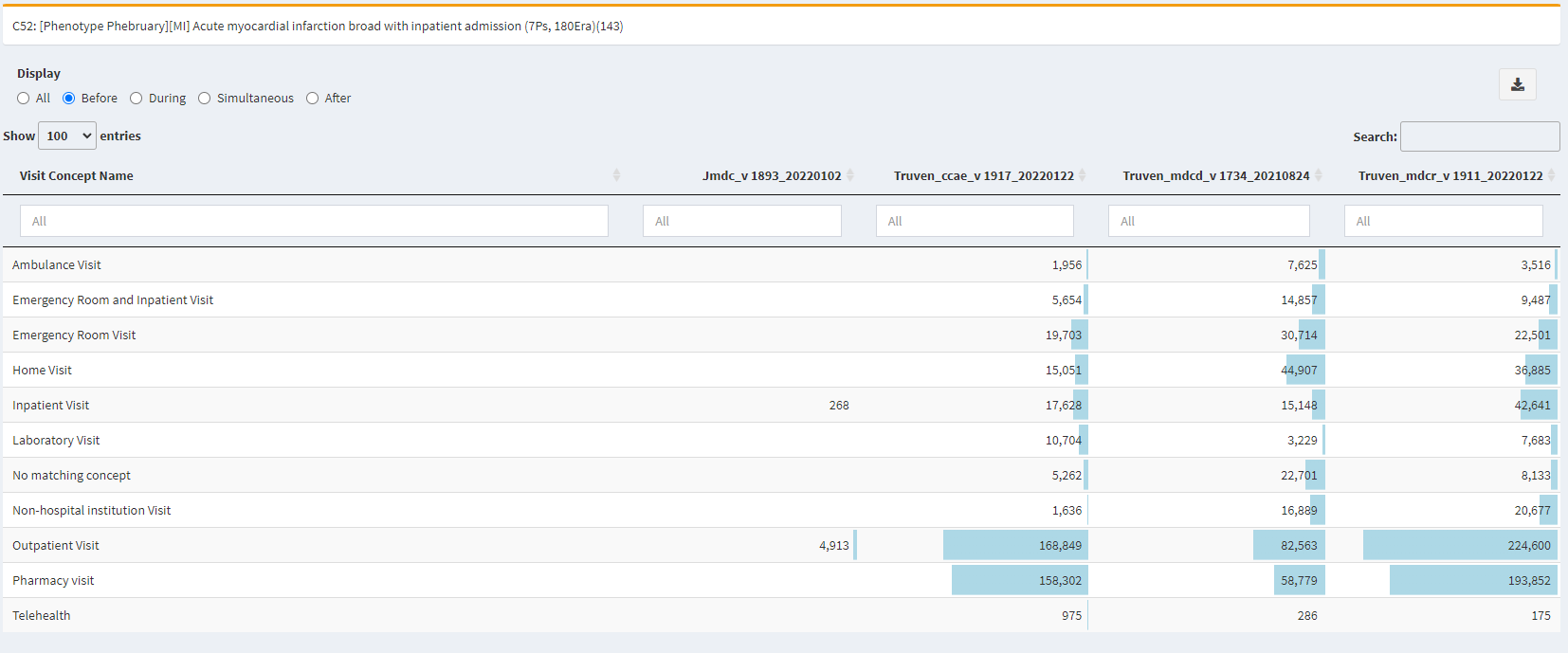
In ARES for the Truven CCAE datasource - i see for
Subsequent non-ST segment elevation myocardial infarction a pretty stable temporal pattern
There is decline in
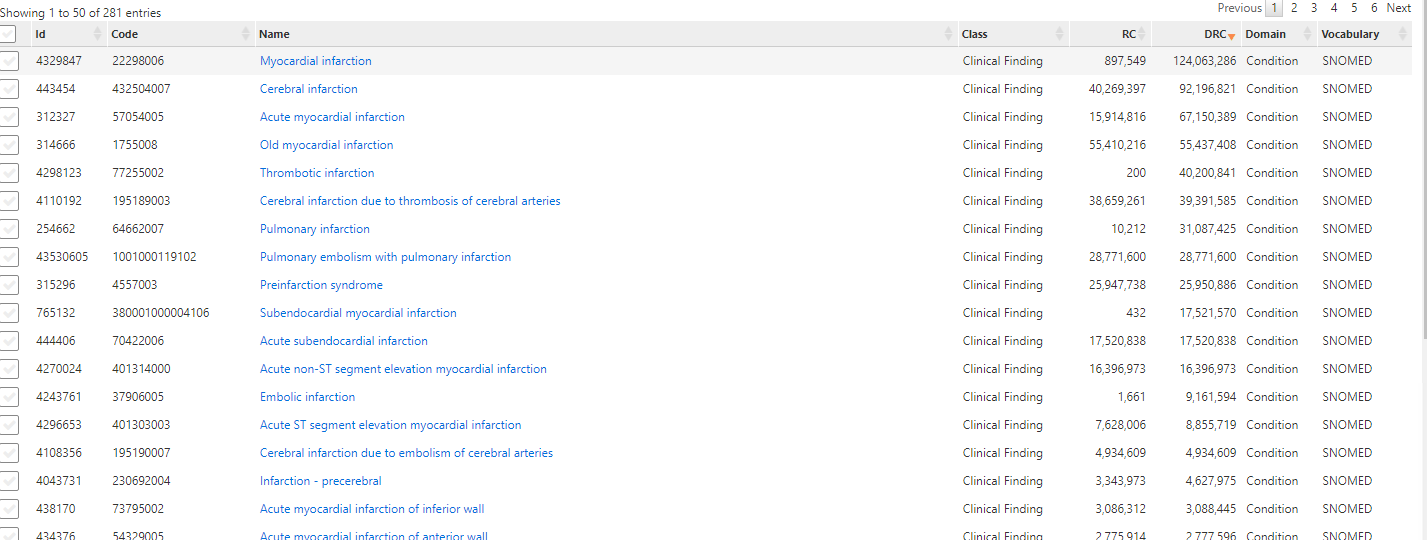
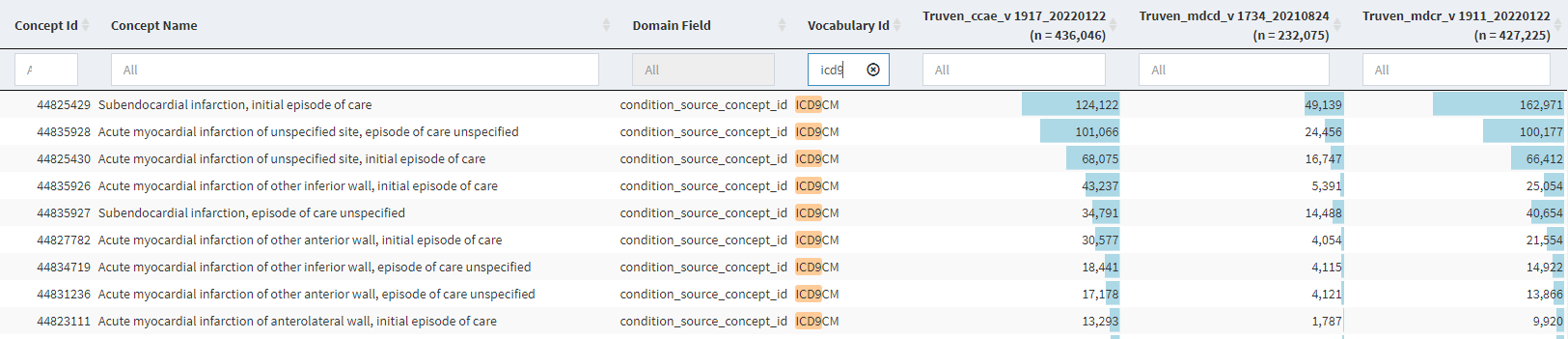
Across the OHDSI network the counts are low for the subsequent code - but not insignificant
compared to the full set
Notice: the counts for old MI - they are pretty large compared to the subsequent codes
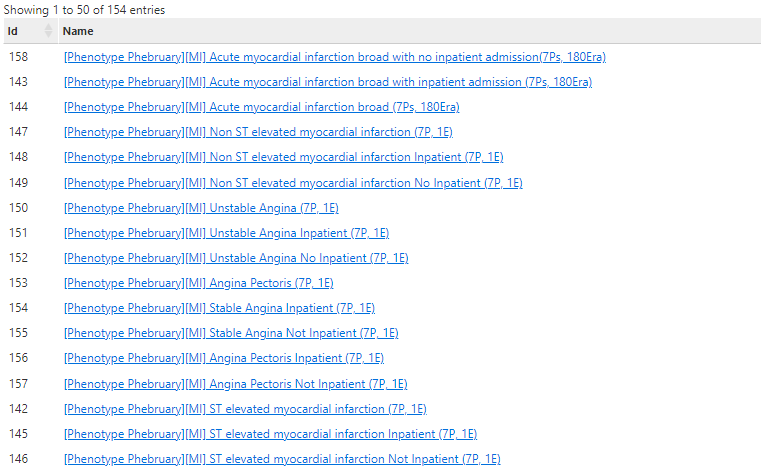
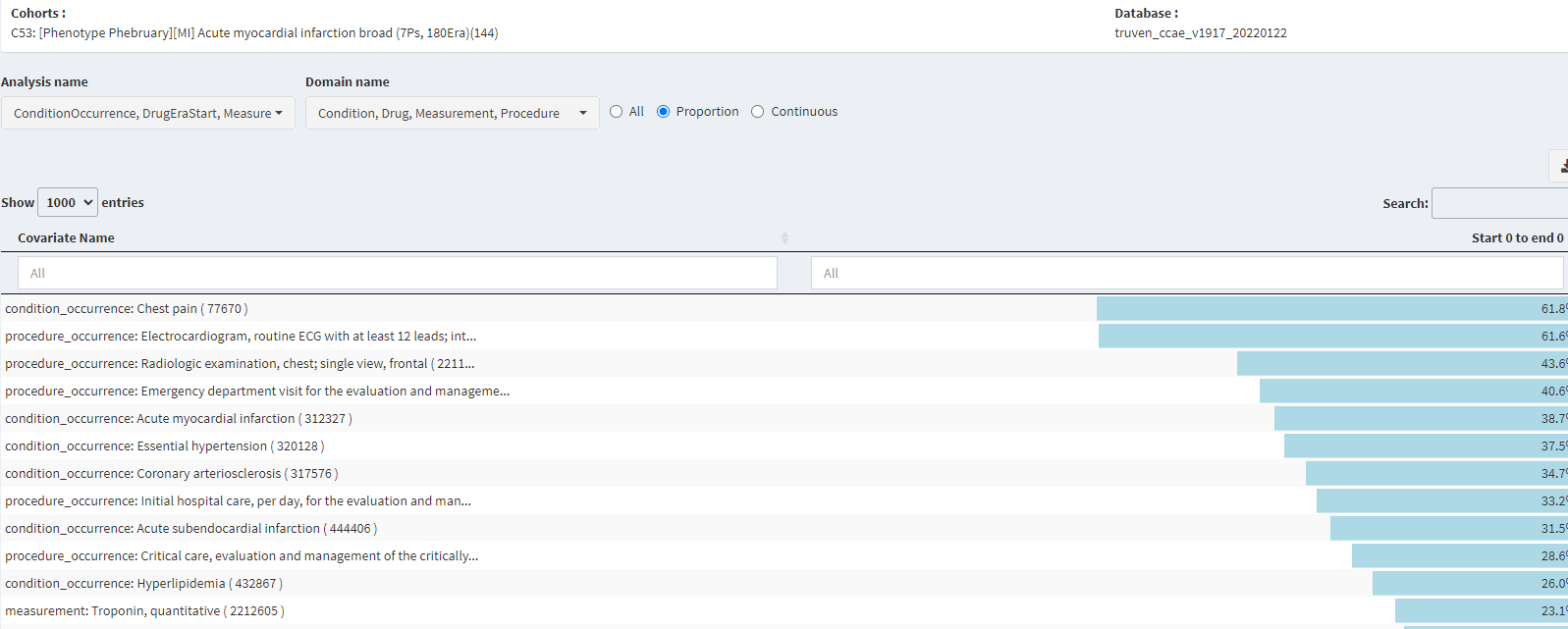
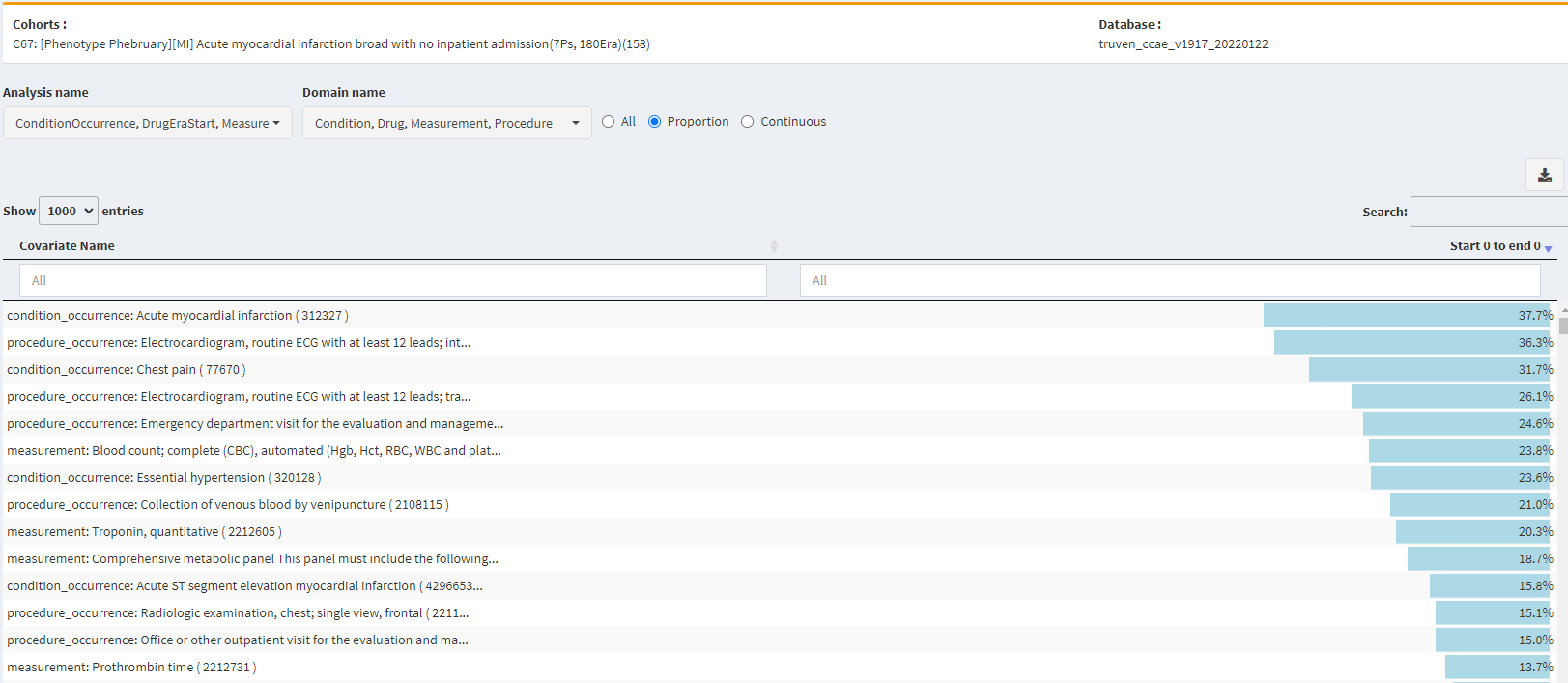
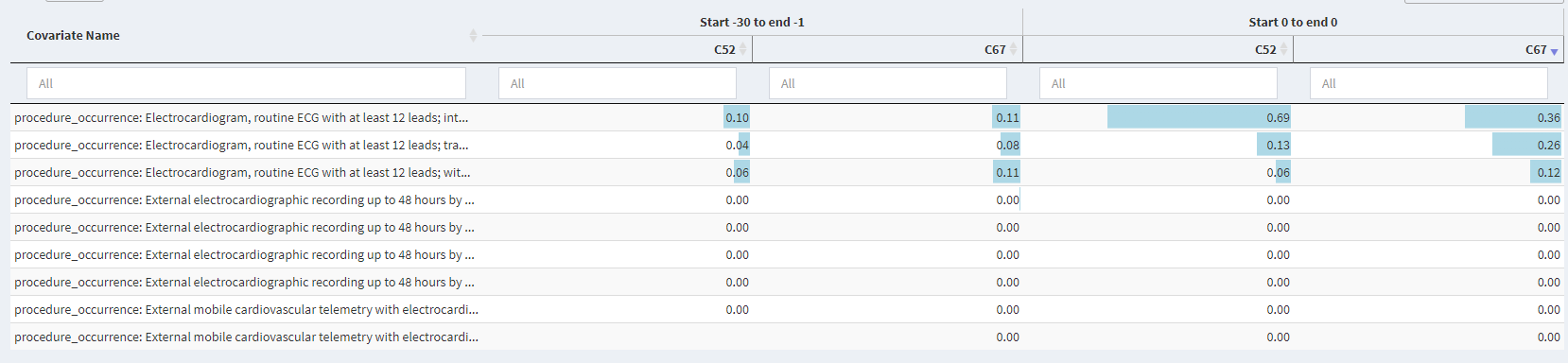
Evaluation of phenotypes for Acute Myocardial Infarction

Insights on sensitivity errors:
Angina
Chest Pain
Next steps:
Evaluation of phenotypes for ST Elevation Myocardial Infarction
(reserved)