@msuchard@schuemie and I are looking at a PLE question for HIV patients. We’re experiencing some challenges with the creating an appropriate concept set for HIV coding.
Is there anyone in the OHDSI community doing HIV research? Anyone have HIV cohort definitions they could share? We could really use help!
@krfeeney, I assume you said this to get me involved? I don’t have an HIV cohort definition offhand but could come up with one fairly easily and would love to get involved.
Yes! End of the semester course work is interrupting my progress for a couple weeks, but we’re eager to hear what you all are doing and hope to have something to show in a month or two.
Happy to share–can you give me an example of the kinds of cohorts you’re trying to find? I’m the slacker that’s been sitting in the back of the class and is a little behind.
Here’s one cohort… but we think this may not be the right order of logic and/or the coding is too restrictive.
Initial Event Cohort
People having any of the following:
a drug exposure of Atorvastatin2
for the first time in the person’s history
with continuous observation of at least 180 days prior and 0 days after event index date, and limit initial events to: earliest event per person.
Inclusion Rules
Inclusion Criteria #1: NoPriorStatin
Having all of the following criteria:
exactly 0 occurrences of a drug exposure of AnyStatins1where event starts between all days Before and 1 days Before index start date
Inclusion Criteria #2: ProteaseInhibitor
Having all of the following criteria:
at least 1 occurrences of a drug era of ProteaseInhibitor4where event starts between all days Before and 0 days After index start date and event ends between 0 days Before and all days After index start date
Limit qualifying cohort to: earliest event per person.
End Date Strategy
Custom Drug Era Exit Criteria
This strategy creates a drug era from the codes found in the specified concept set. If the index event is found within an era, the cohort end date will use the era’s end date. Otherwise, it will use the observation period end date that contains the index event.
One possible thought–if you’re searching for Protease Inhibitors using ATCs, many patients take fixed dose combinations, which are harder to code for ATCs (since the PI will only be part of the therapy). Have you checked to see if you get patients when you look just for that code?
I’m a Co-I on study that meets your 2+ source definition: COMpAAAS Tripartite. The three sources are the Antiretroviral Therapy Cohort Collaboration (ART-CC) which itself is composed of many - mostly European - sources, Kaiser Permanente, and the Veterans Healthcare System (VA). Interoperability hasn’t been top of mind despite my advocating for its value. That might change as progress is made toward shared analyses. Each part has been concentrating on analyses using it’s own source so far. Let me know if you want to me to investigate who you might talk to about working on CDEs that meet study needs.
Do you have any experience comparing cohorts defined with good PI codes vs those that skip PI codes altogether? In other words a comparison that tests the assumption that nearly everyone with an HIV diagnosis is on a PI.
Interesting question–I had assumed PI was of interest for interactions between statins and PI, specifically. But if PI is intended to be a proxy for HIV infection, it’s probably not a very good proxy–I think efavirenz remains pretty popular, and there are lots of other drug classes that are used as the backbone of ART.
Your assumption about the interest in the interaction was correct. That answers the question and - betrays my ignorance about the variations of ART.
The person who question motivated all this is a colleague with drug development background. She would have known. I just wondered whether we could safely avoid the trickiness of representing PI properly. Thanks.
Sorry for the late reply, I Just joined the forum.
Yes, we are looking for HIV patients on PI + statins to study the interaction between the two. So the question @Andrew was asking is pertinent to our analysis.
I have question to a drug expert (Anna O.?) (and fellow HIV experts) @aostropolets
INTRO:
SNOMED CT links SNOMED CT ingredients to SNOMED CT drug classes. I like that A LOT!
I have to do more hoops accross terminologies (and joins prone to mistakes) to do that on the standard drug terms side.
EXAMPLE:
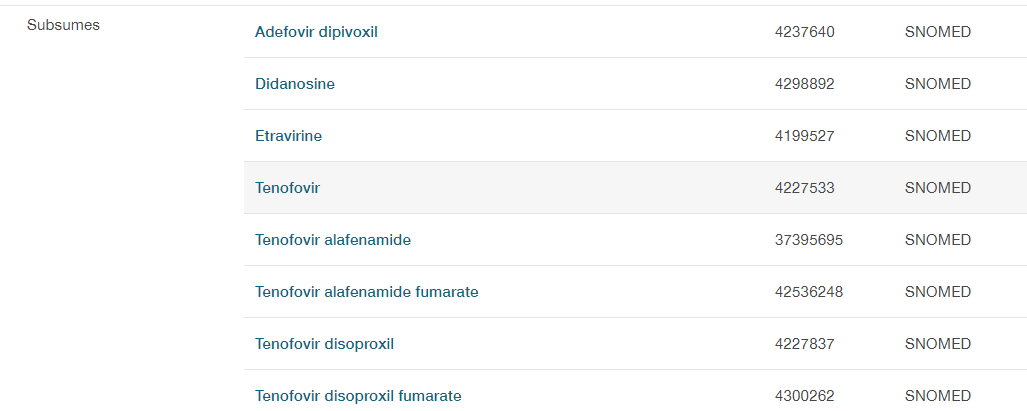
This standard RxNorm term here tenofovir disoproxil Athena
My HIV (and drug) question is: How can I define a cohort of patients on reverse transcriptase inhibitor ? (this NON STANDARD term Athena )
I realize I am walking the hierarchy in the non standard terms - but is the solution to use ATC on the standard term side? And if yes, how exactly (in Atlas)
I also like this Retroviral protease inhibitor class here Athena
(so how do I do the correct jumps (or more ideally, would not have to and Atlas will help me not to make a mistake)
I don’t need a full solution to a thorny problem. Just some/any advice would be great.
I am basically defining my cohort here http://www.ohdsi.org/web/atlas/#/cohortdefinition/1770613 and want to enter something super smart here (note that my CDM does not have drug_eras generated and I must use drug_exposure:
Reverse transcriptase inhibitors belong to J05AF class in ATC, which you can use to get all RxNorm drugs that go under this ATC class.
I added J05AF and J05AE to your concept sets in your cohort, so you can use them.
So it seems like you can use ATC for these purposes, although I’m not sure that this is exactly what you need… Is it?
I have a community question (within HIV research) for sites with full laboratory data.
In one database, we are seeing two LOINC codes being used for HIV 1 viral load.
They both measure “HIV 1 RNA [#/volume]”.
Over time, there does not seem to be a shift from one to the other.
I would be curious to see if the same issue in mapping to LOINC (2 codes being used equally) is present at other sites.
In our diagnostic pathway set of coordinated phenotypes for HIV Descriptive Study, having an accurate set of codes (and corresponding threshold values) is important to us.
In fact, in LOINC terminology, there are also versions of the test where the scale is [log#/volume] and we would need to convert those. Our data don’t have any log versions of the tests but if other sites have it, that is important to consider. (see some of the in this LOINC group concept https://r.details.loinc.org/LOINC/75622-1.html)
For example you can reply with a list of few LOINC codes you seem to be mapping to at your site. (just enumeration of them [no usage numbers]) (or reply to my email)
I’ll look into this at our site and get back to you.
I’m surprised that you don’t have log VL.
That was the way we always got VL values a few years ago when I was involved in a large prospective epi study. Clinician researchers leading that work said it was the standard form at the time and was assumed if not explicitly indicated in test results (2002-2004ish).
 I don’t have an HIV cohort definition offhand but could come up with one fairly easily and would love to get involved.
I don’t have an HIV cohort definition offhand but could come up with one fairly easily and would love to get involved.