We would like to introduce a new workgroup focussed on the development of methods and software for calculating healthcare resource utilization and costs. We are seeking individuals who would be interested in joining this workgroup and are looking for feedback from the community. Thoughts and ideas collected will be shared in this thread or in related thread.
This initiative aims to support the need for descriptive summary statistics for use cases in Health Services Research. Our special focus is on health economics, health insurance, actuarial and financing use cases that have not been the traditional strong suite of OHDSI. The output of the workgroup will be specifications that will facilitate building software tools that augment current OHDSI capability for cohort characterization by incorporating into tools like Atlas ability to perform health economic and health services feature extraction from a cohort. Once completed, this will allow researchers to produce a standard set of tables with certain degree of customizations.
@Gowtham_Rao,
I’m not an expert of health economics. But I’m really eager to participate global study analyzing the medical cost.
Thank you for the contribution.
To create a framework for the conversation, we wanted to introduce and build consensus around the following concepts. Please provide your feedback on these concepts/rules.
1. Evaluation/Target cohort vs comparator/outcome cohort: An analyst will be able to select one or more cohorts for characterization. One of the selected cohorts will be the comparator cohort, and all other cohorts will be the evaluation cohort (s). Evaluation cohorts will be compared to comparator cohorts. Differences between the evaluation and comparator cohorts will be calculated using measures such as standard difference. 2. Index period or Day 0: Cohort start date will be the index period or Day 0. 3. Cohort period: Interval period as any time interval between a subject_id’s cohort-start-date and cohort-end-date, including both dates will be the cohort period for that subject_id. 4. Baseline period: Interval period as any time interval prior to (not including) cohort start date, and going as back as the beginning of the subject_id’s first observation_period_start_date, and in the persons observation period. 5. No overlaps: As a rule, an analysis will have to either belong to the cohort-period, or the baseline period – there will be no overlapping periods that cross over from baseline period to cohort period. 6. Time series However, analysis maybe divided into discrete intervals of time for use in temporal/time series analysis. Time periods may be divided based on a) Relative time period (every 1 day, 7 days, 30 days, 90 days, 180 days, 365 days), or b) calendar period - (every calendar week, calendar year-month, calendar year-quarter, calendar year), or both.
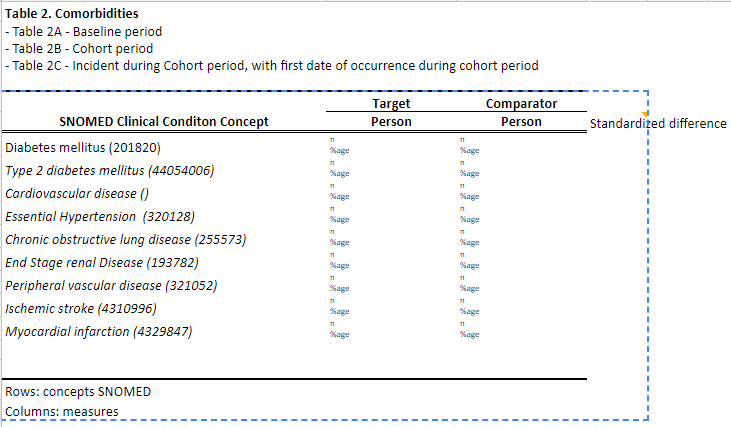
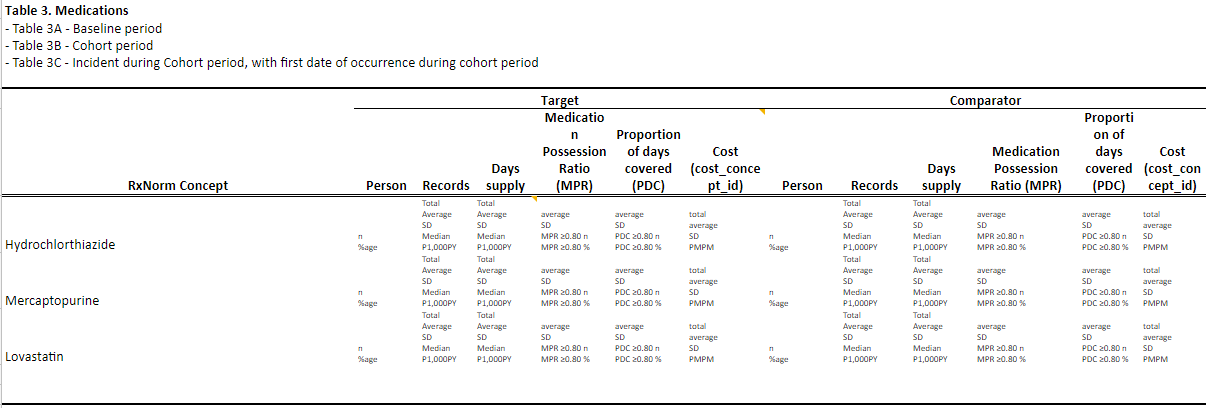
We have created preliminary table shells that illustrate the proposed final product of the analysis. For most of these tables, we propose three sub-types
A. During baseline period
B. During cohort period
C. Incident during cohort period.
The tables include: Table 1: Patient demographics – age, sex, index year, exposure time Table 2: Co-morbid conditions based on SNOMED concepts, includes person count, record count Table 3: Medication use based on RxNorm concepts, includes person count, record count, cost Table 4: Risk scores include Deyo-Charlson, Diabetes Complication Severity, and CHADS-2, along with other scores published using the PLP methods. Table 5: Medical service utilization with costs.
How about adding function to compare the cost on the treatment?
When we compare the cost between target vs. comparator cohort (eg., phenytoin cohort vs. levetiracetam cohort),we can compare the cost for the medicine itself (we can calculate whole cost for phenytoin and levetiracetam in the cohort by using ‘including concept_id for treatment cost’ function to the cost estimation package).
Since levetiracetam is more expensive than phenytoin, I want to compare the expense of the treatment, too.
@SCYou this would be an important question to tackle. When comparing costs between two or more groups (target(s) vs comparators), I can think of the following options
Global cost comparison (pretty straight forward)
Subset of costs comparison, by sub-setting cost records by some rule. (this is what you proposed - sub-setting by RxNorms linked to cost table)
Subset of costs seems to also have two different sub-types
Similar subsets, where the same sub-set rule is applied on records of the comparison cohorts; e,g, comparing costs with the same visit_concept_id, or place_of_service_concept_id, or drug_concept_id
Dissimilar subsets, where different sub-set rule is applied on record of the comparison cohorts e.g. comparing phenytoin costs vs levetiracetam costs - they are not the same RxNorm concept-id’s.
Dissimilar subset cost comparison may be further of two types
Within the same domain - e.g. comparison of drug costs to drug cost (your example)
Between domains or combination of domains eg. cost of surgery vs pharmaceutical intervention
@Gowtham_Rao
This framework is awesome. I can see how much you are familiar with existing OHDSI study pipelines and ecosystem.
In Korean claim database, we have an information for the individual economic status on decimal basis (I stored this information in the observation table). So we can show the basic economic status of the individuals. I’m not sure other databases also has this information. please just keep this in mind.
It would be wonderful if we show whole medical expenses before the cohort_start_date, during cohort date, and after the cohort_end_date. and mortality, too.
Then, I think we can do simple analysis for the cost-effectiveness of the drug, device or procedures.
Again, I think this work is really necessary for OHDSI. And I’m so grateful to you for the contribution.
Should we keep the established terms “Test Cohort” and “Comparator Cohort”? Otherwise you will confuse a ton of people if you call them “Comparator” and “Evaluation”.
Thank you for picking up on that. We will need some guidance on this topic from the community - because we (or atleast I), am confused because we seem to use these terminologies inconsistently.
Today the workgroup mocked up the output for the cost and utilization. We also wrote some pseudocode. Please review and provide input for this document
Tomorrow we will mock up the user-interface for Atlas
If you would like to join the workgroup and assist in the development, please post in this forum
Hey everyone! Nataly here from J&J. we do health outcomes research for medical devices in our studies and was wondering about the update of this workgroup. I would love to help and learn as much as I can to help implement it in our projects and help others do the same. Please let me know how I can participate.
Hello, @Nataly_Patino
Could you tell me which kind of database you can access? I’m working on Korean National claim database for cost and survival trend in cancer patients and looking for the collaborators.