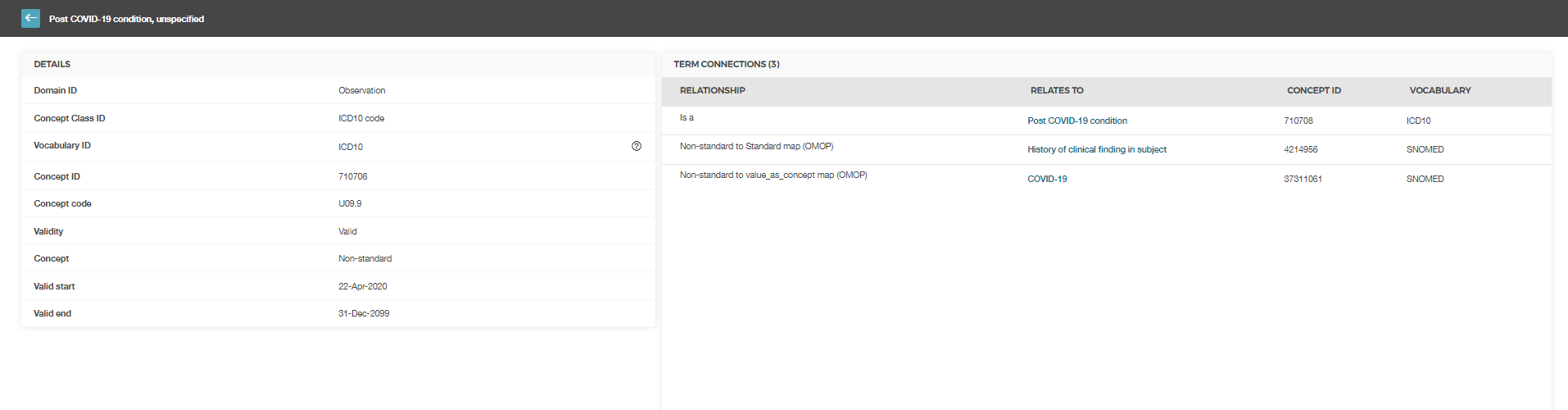
The ICD10CM code for “long COVID” (U09.9 Post COVID condition) is required to support research use cases in N3C. Current non-standard concept mapping provides a standard concept that is is too far up the hierarchy to meet the semantic needs for any research use cases
The only clinical fact this code captures is historical COVID-19.
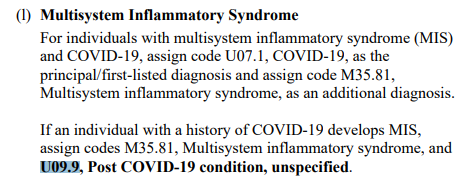
It’s explicitly stated for the Multisystem Inflammatory Syndrome - the actual manifestation of the long COVID should be coded separately.
It’s not so clear for other manifestations, but supposed to be the same - doctors define the relation on their own.
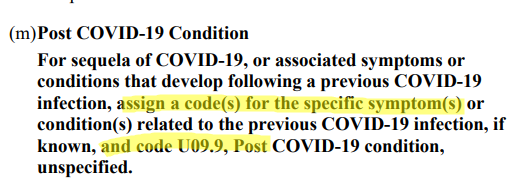
Given the fact the long-COVID criteria were blurred, we tried not to impute the facts out of doctors’ suggestions and would recommend researchers to capture the post-COVID the same was: History of COVID + manifestations of its actual sequelae.
But I agree that by some other coding practices one will capture only the fact of sequelae using the code like that. So it comes to the question of whether: (a) such coding practice exists; (b) long-COVID criteria are defined enough and we believe the relations like that.
To support the coding of terminology used to describe prolonged symptoms following COVID-19 illness, we propose the following OMOP Extension concepts in Condition Domain with suggested definitions according to current guidelines on the management of long COVID:
Sequela of COVID-19 - persistent symptoms and/or delayed or long-term complications of SARS-CoV-2 infection beyond 4 weeks from the onset of symptoms
1.1. Long COVID-19 (Syn: Chronic COVID) - subsumes persistent symptoms and/or delayed or long-term complications of SARS-CoV-2 infection beyond 4 weeks from the onset of symptoms excluding ICU-treated patients.
1.1.1. Ongoing symptomatic COVID-19 - signs and symptoms of covid-19 present from four weeks and up to 12 weeks
1.1.2. Post COVID-19 syndrome - signs and symptoms that develop during or after an infection consistent with covid-19, present for more than 12 weeks and are not attributable to alternative diagnoses
1.2. Post COVID-19 intensive care unit syndrome - constellation of symptoms involving physical strength deficits, cognitive decline, and mental health disturbances observed after discharge of patients from critical care units that persist for a protracted amount of time.
Hierarchy of proposed concepts is defined by numbering. @Christian_Reich@Alexdavv@Dymshyts
thanks for creating a respective github issue. This will help us to keep track of this.
How do you like the proposal, which I understand, is to identify patients with long / post CoViD syndrome by some sort of hierarchy: sequelae as a parent and two (three) possible children: long CoVid with a medium / long duration and post ICU syndrome (due to CoViD19)?
I would not try to be more specific, because we are at this time not really in the position to define OMOP extension concepts that summarize a whole lot of attributes. I would presume we are still in the process of defining Long CoViD and this term will be filled with your meaning over time, hopefully helped by us. Yes, we have fairly solid knowledge of a couple of attributes that seem to be related to it (e.g. WHO also seems to use ICD10 code G93.3 – post-viral fatigue) and we know there is “brain fog”, lung damage with shortness of breath, ongoing inflammatory symptoms and some other less well defined effects. When it comes to data, wouldn’t it be a job for a phenotyping crew to define a particular Long CoViD classification as a concept set / cohort?
So, yes, it probably makes sense that the equivalent to a high level clinical decision can be stored, where a physician has decided that a patient is suffering from one of the above variants. Is that your intention?
Hello Mik & everyone… Here’s an illustration which supports our use case. The very researchers that will define the nature and etiology of the “long COVID” condition are the ones that are making this request. We cannot predict the future. Likely this will not be the last time emerging science will need support from the OMOP community. The need is to develop a nimble vocabulary management process which supports the motile nature of scientific discovery
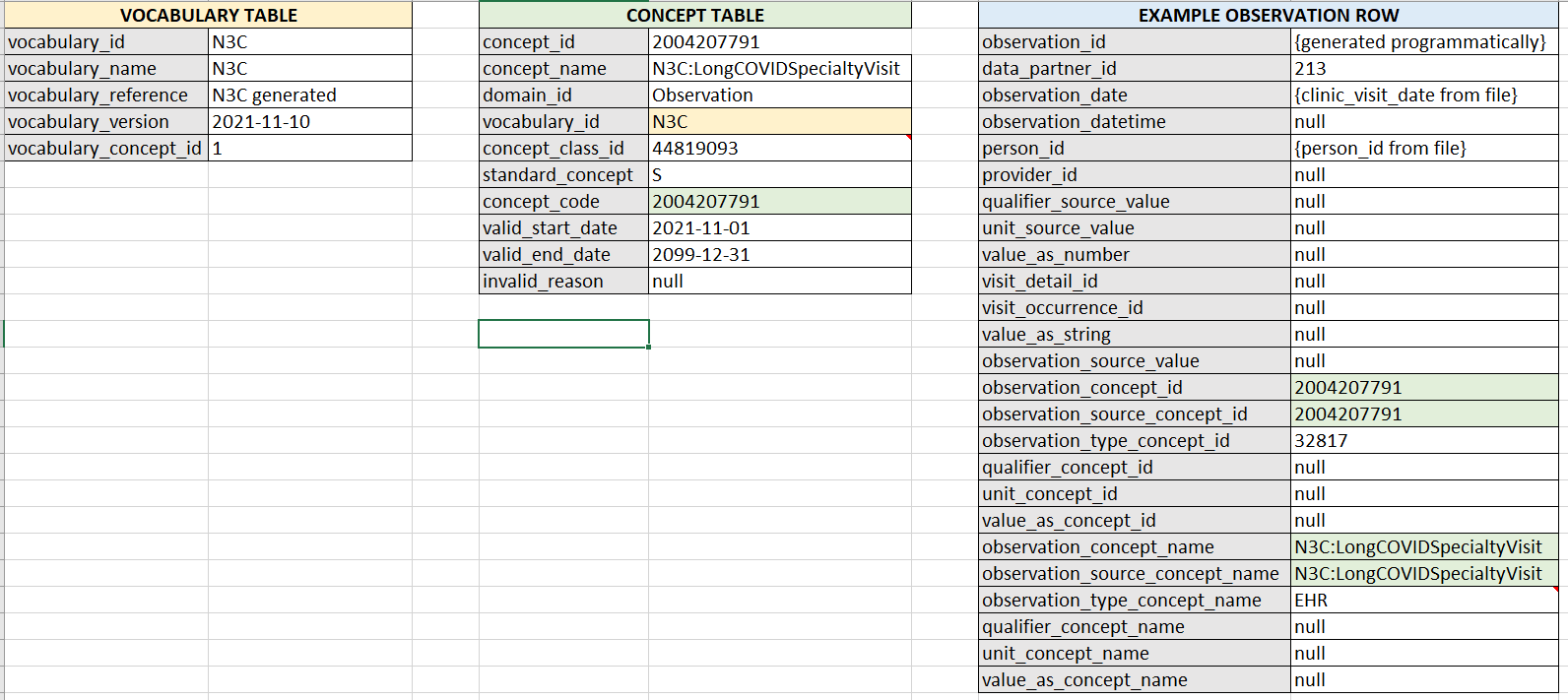
Here’s a copy of the extension Stephanie created based on the N3C / RECOVER project group discussion and needs that we discussed in our small group chat today
Hi,
from our discussion, I understand the use case is that a particular in-/outpatient visit is present in the source data that is connected to long CoViD in a patient. We are not entirely sure if this is a particular clinic visit or just a visit of a patient suffering from long CoViD.
Until a proper target concept exists in one of the general terminologies, we propose to create only the 1.1 concept (Long COVID-19 syndrome) to cover this immediate need as an observation concept.
We also concluded that it is time to open a new chapter in the COVID-19 instructions wiki for Long COVID and SARS-CoV2 vaccinations.
It may be confusing if we add a bucket code, but not the one that is supposed to be it. I’d suggest to stick to the SNOMED hierarchy and principles picking the “1. Sequela of COVID-19”. Otherwise, we’d need to map everything (Post COVID, ongoing COVID, Post ICU) to the long COVID concept that doesn’t sound completely clean.
Are we capturing a visit or condition? If condition, what’s the rationale behind the Observation Domain?
Per our discussion today, I want to make sure our written discussion decouples two parallel things:
“Long COVID as a condition” aka the need to phenotype Long COVID – this is a systematic way to qualify patients as “Long COVID syndrome” based on the clinical attributes that are present at that point in time in their health records. This is being done by @Gowtham_Rao@Evan_Minty@annika_joedicke and team in the Phenotype WG Long COVID subgroup.
Ontological representations of terms that are associated to Long COVID related clinical attributes that are not currently picked up in our CONCEPT table but are in terminologies we support OR can be incorporated in the OMOP Extension structure temporarily while we “wait”.
To clarify, the table above represents 2 - where Stephanie is creating a CONCEPT record to record Patients who are seen at a Long COVID Clinic. It is not the same as rubberstamping someone as “having had long COVID”.
This is a bit of a meandering thought as the title of this thread is related to ICD10 codes. The ICD10 codes that came out are different. (My impression is that these ICD10 should be treated as local clinical codes entered in an EHR by someone who is indicating that person is in their office for a Long COVID encounter – whether they are in a long COVID clinic or not.)
The Long COVID clinic visit is the confirmed presence of a clinical encounter that is specific to specialty care for those who are suspected to have long COVID. It, in itself, may have clinical noise in that there are different protocols for how people show in long COVID clinics depending on the clinical practice patterns of that specific medical center. The RECOVER program is working with a subset of sites to identify if they have a long COVID clinic that qualifies patients for the presence of this encounter type and then is providing ETL guidance by data model as to how to send that information so it gets standardized to this particular concept.
Why this is important to delineate: @DaveraG presented a use case about the ambiguity of coding related to HIV/AIDS in the 1980s before we knew what HIV/AIDS was. This use case may have eventually congealed around clinical definitions for what constituted HIV/AIDS. However, the period of time when we did not know the clinical attributes that fed into HIV/AIDS is not a clinical coding issue where we have no ontological representation of the terms from the clinical encounter. Instead, the period of time when we did not have clinical consensus on what constitutes an HIV/AIDS diagnosis (because we also may have not understood or seen all of its manifestations in a way that we could code it accurately) is a phenotyping problem.
I would caution that we keep this in mind as we continue to tackle this issue. There are 25 symptoms in the WHO Delphi Consensus on Long COVID. If people are interested in ensuring we have robust concept sets for these specific concepts, you may join the Phenotype WG tomorrow from 12:30-5:30PM EST as we do a hackathon to do design diagnostics in PHOEBE and ATLAS. You can participate via MS Teams in the Phenotype WG group or directly connect via this MS Teams Invite Link. Note if you are not in the Phenotype WG group of OHDSI MS Teams, you may have issues in accessing the collaboration sheet. Please use the onboarding form at OHDSI.org to be added to this area.
Path of least resistance. It’s a visit type not a condition.
Observation was the least offensive place to temporarily hold this concept while we better understand the intricacies of what sites can ETL and what they have available in their source systems. We would like to upgrade it to a visit_concept_id at some point but we are taking baby steps. We’re already harassing @Christian_Reich about the need to make this a real kind of specialty clinic visit concept.
I second this As we discussed yesterday in the EHR WG call, the standard concept_ids in the Visit domain are notoriously limited in coverage & granularity. Currently, I suggest researchers use a combination of the care site, provider, dates and other attributes to define these long/chronic covid visits. If there was a standard visit concept_id for this, then the pre-processing can be done during the ETL. Isn’t that the OHDSI way? To quote the famous @Christian_Reich “put it on the ETL smucks”
And to be clear, we know that there’s a LOT of guess work being done at the site-level to figure out “who was seen in the Long COVID clinic” because it’s not easily captured. We can absolutely use the RECOVER sites to help figure out ETL implementation guides and best practice.
It will not be one size fits all but we can deduct how we get to a pre-processing stage. @mgkahn has been one of our first navigators of this tortuous journey. I am sure he will gladly share with the tribe the tribulations of pioneering this.
With respect to the Long Covid condition: This is not easy. We are stuck between the rapid speed of clinical research (and obviously the high urgency on this particular issue), and the slowness and contradictory nature of definitions evolving as we speak.
The solution is (you knew I would say it!) in the use case:
If we want to create phenotypes of this condition - we don’t need anything. Long Covid becomes a cohort definition.
If we believe the community has settled on a set of precisely defined conditions we should adopt something like @Mikita_Salavei’s mini-hierarchy.
If we believe this is a moving target folks will not have a common clear understanding no matter what the various authorities @mik listed state, we should create one catch-all concept.
I would strongly suggest we go by 3. And you seem to have concluded likewise. This concept could be called sequalae, long, post, or any of these as synonyms. Whether or not there are differences in the patterns justifying the creation of different conditions will be the output of the research, not the input.
Regarding the Long Covid clinic: Visits are configurations of clinical care, where the main attributes are (i) does the patient come to the provider or the other way around, (ii) does the patient stay in bed over night and (iii) is the healthcare a focused activity or is there a permanent service available to intervene any time. All this is from the patient perspective, not the perspective of the provider.
In this case, you have to explain how a Covid clinic is any different than an outpatient visit. The nature of the disease is not sufficient to draw the line. Something else has to be substantially differently organized.
So, it might be a sequela or a long covid, there are several definitions.
So, what if we create an OMOP Extension concept, call it “Post COVID-19 condition” and map ICD10CM to it?
I would stick to the ICD name because it exactly describes this bucket code.
Then if we see in the data something like @Mikita_Salavei described, we can add that later as descendants of the “Post COVID-19 condition” concept.
Now I see the point around the Observation domain. Why don’t we call things by their names then?
We have a separate hierarchy of suspected conditions under the Observation domain here and suspected COVID sequela can become a part of it.
Pointing out to the similar discussion we had about COVID…
So it seems the only question is whether we already want to distinguish suspected and “confirmed” sequela of COVID by having 2 separate bucket codes.
Sure, but we want it to be crystal clear so users don’t mix it up with any of @Mikita_Salavei’s definitions. Especially considering the moment we’ll be adding these all to the vocabulary. This clarity will support future changes in the terminology and related ETL/mapping adjustments.
…as well as any condition that developed following a previous COVID-19 infection.
This one conflicts with one of @Mikita_Salavei 's definitions.
This is supposed to be a level 3 code, not the top guy. While ICD10CM, in fact, is just a history of COVID-19 and the most assumption we can do is mapping to “suspected COVID sequela” (if we believe it deserves a separate concept).
Exactly! Something is happening not necessarily but presumably connected to previous COVID. While something is coded separately, this U09.9 code is somewhat in between:
the history of COVID (for the MIS case it’s clearly stated in the coding guidance).
suspected COVID sequela.
But what would be a landing target if this is basically an OR statement?
Well, ICD10 code doesn’t include Ongoing symptomatic COVID-19, right?
So that’s the difference?
Again, there’s an EHR code and in most of the cases that’s the only available information.
And let’s say, someone have a history of COVID, then they got hit by a car got a brain trauma and got loss of smell (not post covid condition)
and someone else also have a history of COVID but wasn’t hit by a car, but lost smell as well (post covid condition).
Obviosly for the COVID research I need the second patient. and this “Post COVID-19 condition” code is what I have only. So we need that code as target you like it or not.