In this thread, @Khyzer_Aziz will be leading us thru his teams experience going through Phenotype Development and Evaluation Process for Neonatal Hypoxic Ischemic Encephalopathy. This is anticipated to be a month long process. As he progresses he has agreed to make posts on this thread to describe his experience.
Week 1: we hope to have the target clinical idea described and have built 1 or more candidate cohort definitions.
Week 2: we attempt to instantiate the cohort on one or more data sources, and run CohortDiagnostics on it. Post the results in public domain.
Week 3: we will review the output from one or more data sources, and perform and evaluation. Based on the evaluation - we might revise the cohort definitions.
Week 4: we finalize the cohort definitions and have an evaluation document. This evaluation document can then be peer reviewed by the community. If accepted the phenotype will be then added to the OHDSI Phenotype Library.
Thank you @Khyzer_Aziz for taking this challenge on a tight timeline. We are all learning together and our goal here is to test and harden the best practices proposed by the OHDSI Phenotype Development and Evaluation workgroup. @Khyzer_Aziz and @Evan_Minty will work together as Phriends!
Thank you @Gowtham_Rao. Challenge accepted! I am excited to be a part of the OHDSI community and engage so many new Phriends to help with this work!
As a neonatal intensivist and clinical researcher, I am focused on improving clinical decision-making for patients, families and clinicians utilizing a precision medicine approach. Neonatologists, pediatricians and internists are encumbered by both a lack of early identification of neonates at risk for brain injury and treatment therapies. There is a LOT of clinical and basic science research that shows what happens in the fetal and neonatal stages has a lasting impact on brain and total body health for the entirety of a person’s life. Hypoxic ischemic encephalopathy (HIE) is one of the most common type of brain injuries in newborn babies. Our NICU Precision Medicine Center of Excellence is focused on improving outcomes for HIE, a multifactorial condition.
Let’s take a closer look at this specific type of neonatal brain injury Hypoxic Ischemic Encephalopathy.
Clinical Description: The incidence of Hypoxic Ischemic Encephalopathy (HIE) has been reported as 1.5-2.5 per 1000 live births in developed countries. Among affected infants, 40-60% die by 2 years of age or have severe disabilities (1-4). HIE occurs primarily due to acute perinatal asphyxia – a state where impaired cerebral blood flow and oxygen delivery to the brain result in decreased energy production leading to cell death (5-6). The only approved therapy proven to slow down and prevent energy failure in the brain of neonates suffering of HIE is whole body hypothermia (cooling), which it is initiated within 6 hours after a hypoxic insult (assumed to occurred at time of delivery) (7-9). Cooling reduces the metabolic demands of the neonate which in turn attenuates the deleterious metabolic cascade (and toxins) which cause brain injury (i.e. death or severe disabilities) (6). A neonate undergoing cooling is admitted to the neonatal intensive care unit (NICU) and is typically cooled for approximately 72 hours (7-8,10).
During this time period, neonates are closely monitored in the NICU through clinical exams, labs, imaging (echocardiograms, x-rays, head ultrasounds), and continuous electroencephalogram (cEEG) for complications related to the underlying hypoxic-ischemic insult. Complications associated with cooling include agitation, low blood pressure, pulmonary hypertension, and coagulopathy (7-8,10). After cooling is completed, a neonatal brain magnetic resonance image (MRI) is obtained to visualize regions of the neonate’s brain and identify potential areas of damage.
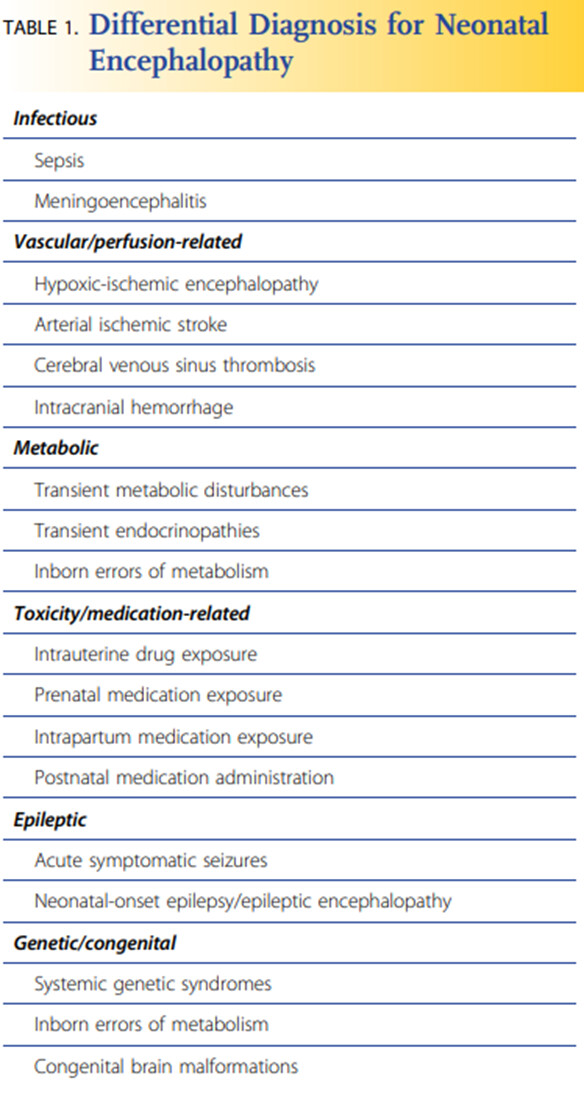
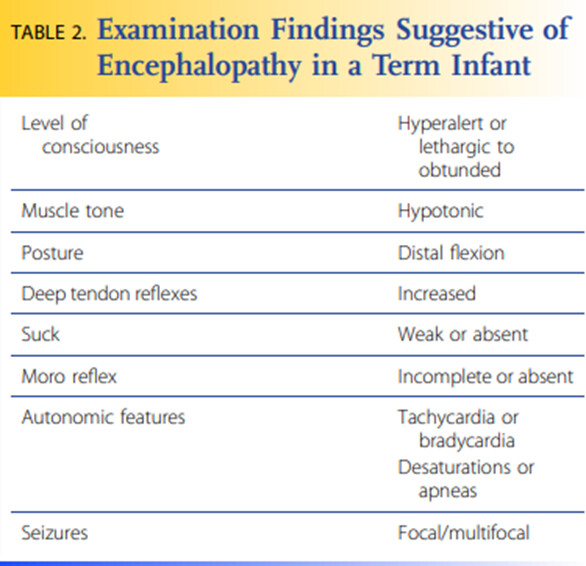
In NeoReviews, a journal published by the American Academy of Pediatrics, Russ et al. provide tables that include the differential diagnosis for neonatal encephalopathy (Table 1), the clinical presentation of neonatal encephalopathy (Table 2), and the diagnostic evaluation for neonatal encephalopathy (Table 3) (11). As seen in these tables by Russ et al., there’s ample opportunities to define and build this HIE specific neonatal cohort. One unique feature differentiates HIE from the all other conditions listed in Table 1, HIE is the only neonatal disease that receives whole body hypothermia (cooling) as part of the treatment/management paradigm.
References:
Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE, McDonald SA, Donovan EF, Fanaroff AA, Poole WK, Wright LL, Higgins RD, Finer NN, Carlo WA, Duara S, Oh W, Cotten CM, Stevenson DK, Stoll BJ, Lemons JA, Guillet R, Jobe AH; National Institute of Child Health and Human Development Neonatal Research Network. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med. 2005 Oct 13;353(15):1574-84. doi: 10.1056/NEJMcps050929. PMID: 16221780.
Lai MC, Yang SN. Perinatal hypoxic-ischemic encephalopathy. J Biomed Biotechnol. 2011;2011:609813. doi: 10.1155/2011/609813. Epub 2010 Dec 13. PMID: 21197402; PMCID: PMC3010686.
James A, Patel V. Hypoxic ischaemic encephalopathy. Paediatrics and Child Health. 2014 Sep 1;24(9):385-9.
Chalak LF, Sánchez PJ, Adams-Huet B, Laptook AR, Heyne RJ, Rosenfeld CR. Biomarkers for severity of neonatal hypoxic-ischemic encephalopathy and outcomes in newborns receiving hypothermia therapy. J Pediatr. 2014 Mar;164(3):468-74.e1. doi: 10.1016/j.jpeds.2013.10.067. Epub 2013 Dec 12. PMID: 24332821; PMCID: PMC4006934.
Graham EM, Ruis KA, Hartman AL, Northington FJ, Fox HE. A systematic review of the role of intrapartum hypoxia-ischemia in the causation of neonatal encephalopathy. Am J Obstet Gynecol. 2008 Dec;199(6):587-95. doi: 10.1016/j.ajog.2008.06.094. PMID: 19084096.
Northington FJ, Chavez-Valdez R, Martin LJ. Neuronal cell death in neonatal hypoxia-ischemia. Ann Neurol. 2011 May;69(5):743-58. doi: 10.1002/ana.22419. PMID: 21520238; PMCID: PMC4000313.
Shankaran S, Laptook AR, Pappas A, McDonald SA, Das A, Tyson JE, Poindexter BB, Schibler K, Bell EF, Heyne RJ, Pedroza C, Bara R, Van Meurs KP, Grisby C, Huitema CM, Garg M, Ehrenkranz RA, Shepherd EG, Chalak LF, Hamrick SE, Khan AM, Reynolds AM, Laughon MM, Truog WE, Dysart KC, Carlo WA, Walsh MC, Watterberg KL, Higgins RD; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Effect of depth and duration of cooling on deaths in the NICU among neonates with hypoxic ischemic encephalopathy: a randomized clinical trial. JAMA. 2014 Dec 24-31;312(24):2629-39. doi: 10.1001/jama.2014.16058. PMID: 25536254; PMCID: PMC4335311.
Laptook AR, Shankaran S, Tyson JE, Munoz B, Bell EF, Goldberg RN, Parikh NA, Ambalavanan N, Pedroza C, Pappas A, Das A, Chaudhary AS, Ehrenkranz RA, Hensman AM, Van Meurs KP, Chalak LF, Khan AM, Hamrick SEG, Sokol GM, Walsh MC, Poindexter BB, Faix RG, Watterberg KL, Frantz ID 3rd, Guillet R, Devaskar U, Truog WE, Chock VY, Wyckoff MH, McGowan EC, Carlton DP, Harmon HM, Brumbaugh JE, Cotten CM, Sánchez PJ, Hibbs AM, Higgins RD; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Effect of Therapeutic Hypothermia Initiated After 6 Hours of Age on Death or Disability Among Newborns With Hypoxic-Ischemic Encephalopathy: A Randomized Clinical Trial. JAMA. 2017 Oct 24;318(16):1550-1560. doi: 10.1001/jama.2017.14972. Erratum in: JAMA. 2018 Mar 13;319(10 ):1051. Khan AM [added]. PMID: 29067428; PMCID: PMC5783566.
Kapadia VS, Chalak LF, DuPont TL, Rollins NK, Brion LP, Wyckoff MH. Perinatal asphyxia with hyperoxemia within the first hour of life is associated with moderate to severe hypoxic-ischemic encephalopathy. J Pediatr. 2013 Oct;163(4):949-54. doi: 10.1016/j.jpeds.2013.04.043. Epub 2013 Jun 5. PMID: 23759422.
Chalak L, Kaiser J. Neonatal guideline hypoxic-ischemic encephalopathy (HIE). J Ark Med Soc. 2007 Oct;104(4):87-9. PMID: 17953198.
I took on this challenge with Aziz. He was called in to a very busy clinical week, so we didn’t get a chance to connect again until this week.
I’m a internist, so I elected to deal with big people, not little people.
Perhaps it’s the act of thinking through the data of little people, that caused me to reflect on what an honor it is to be able to do this work.
Here, when we’re looking to index at t=0, it really is t=0, and it didn’t go as planned for these little ones. I’m very interested in seeing this cohort definition come to fruition, so that we can ultimately see what we might be able to generate in terms of evidence and insights that might help.
From his clinical description, our subsequent discussion, a couple of points of interest:
We expect an HIE code to have high specificity. It labels a case of encephalopathy as effectively having been the result of a complicated L&D, so it may be applied later on in a case, as opposed to right away, and it may take time to rule out other causes.
a. This normally might be a situation where you’d worry about index date misspecification, but in this case, that’s less of a concern, as we will be indexing on the start of their inaugural visit
We also expect ‘induction of hypothermia’ to be highly specific, as noted in the clinical description.
I created 2 cohorts based on those concepts. I found that HIE was applied more often than we see ‘induction of hypothermia’ (at least a factor of 10) across a couple of datasets (CCAE, Premier)
I performed some characterizations of cohorts (condition occurrence of Brain Damage due to Hypoxia, a parent that subsumes HIE, and Induction of Hypothermia). In reviewing those and a limited set of profiles, I also observed that in cases of HIE, we can see ‘condition occurrences’ of hypothermia, which I wondered might be a surrogate for the procedure occurrence.
Kyzer also raised the possibility that ‘treatment of hypothermia’ might even be used, and I saw some evidence of that in the data.
He had also had some success in finding cases at JHU by looking for body temperatures ≤34.5. This wouldn’t generalize to non EHR data sets, but it would be interesting to see how it does in other EHR sets.
In patients that have a procedure occurrence of ‘induction of hypothermia’ about 85% (eg. in CCAE) have an HIE condition occurrence. But 15% have another label applied.
I built out 2 additional concept sets that are more inclusive of other encephalopathies. ‘Brain damage due to hypoxia’ is a parent of HIE, and has many other children that look, semantically like they could reasonably be applied.
I also iterated that through Phoebe, to come up with an even broader set (called ‘Encephalopathy possibly due to hypoxia’. Phoebe suggested conditions like ‘apgar scores’ of 5, 4, and zero – interestingly these are cut offs of clinical significance. I’ve also added more general concepts (with no decedents) after reviewing / discussing with Kyzer.
So we have the following possible components:
Diagnosis
Therapy
high specificity
HIE
Induction of Hypothermia
≥4 Temperatures ≤34.5
Brain damage due to Hypoxia
Condition Occurrence of Hypothermia
lower specificity
Encephalopathy possibly due to hypoxia
Rx of Hypothermia (?)
In the next phase, I suggest we undertake some investigations of these components in Cohort Diagnostics
The goals there will be to :
“Prove out” the specificity of (a minimum of) a single condition occurrence of HIE, or Induction of hypothermia. We could pre specify a number, say 90% as being adequate.
Examine the marginal contributions of the less specific components either
a. In combination with the more specific components, if single occurrences of those aren’t enough , or
b. Possibly in combination with each other, where we are interested in the marginal contribution they would bring that might increase sensitivity, at the risk of degrading specificity.
I also feel pretty confident in assessing at least one candidate as
HIE Dx OR Induction of Hypothermia
And we can sort out what additional contributions the other components may or may not have.
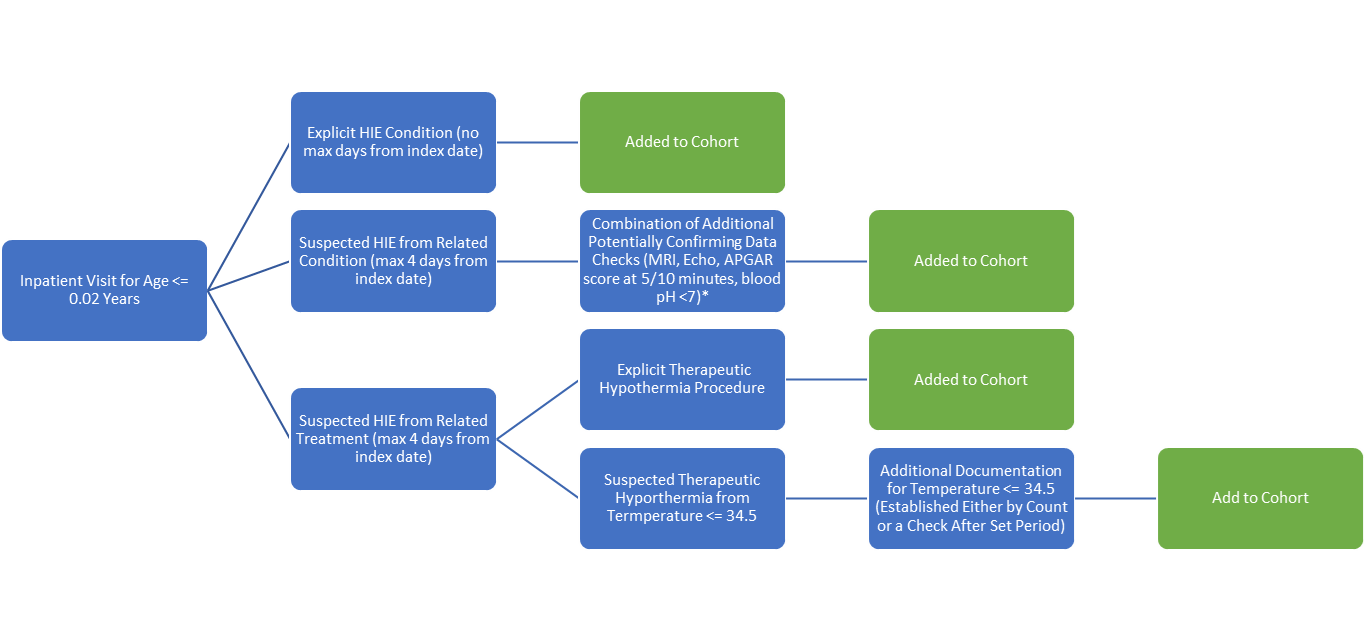
Hi OHDSI community! I’ve been working with Dr. Aziz and a team of others from our OMOP class at Hopkins on creating this HIE phenotype (shoutout to Alfred, Danielle, Dianne, Kristin and Stephanie). Here is a decision tree that represents how we’ve been thinking through creating this cohort:
To start, we look for inpatient visits for patients <= 0.02 years of age, which gives us admissions for neonates within the first 7 days of life. Within that inpatient visit, we look for either an explicitly documented HIE condition, like concept ID 45766189; if we find one, we go down the high specificity branch, and the patient is added to the cohort without additional checks.
We then setup a couple branches to increase the sensitivity of our cohort definition. In one, we look within the inpatient visits for documented conditions that we suspect could be HIE based on documentation for a more broad condition, like concept ID 372887 (Disorder of brain). We then attempt to find other documentation that could indicate HIE; some examples include APGAR score at 5/10 minutes, MRI performed, Echo performed, and a blood pH <7. While currently represented by one box in the above diagram, this will evolve into several additional checks that look for a combination of the various factors.
To further increase sensitivity, we also look for therapeutic hypothermia during the inpatient visit. Since therapeutic hypothermia is only used for suspected HIE, it warrants different considerations that the combination of checks discussed above. If therapeutic hypothermia is explicitly documented as a procedure within 4 days of the admit date, they are added to the cohort. This aligns with the general guidelines for therapeutic hypothermia to be started within 6 hours and to last for 72 hours, while also leaving flexibility for practice that differs from the guidelines. We also looks for a pattern of low temperatures that indicate a patient was being intentionally cooled and remained cold for an some period of time; we are still working on the exact criteria. It is important to check that the period of low temperature was prolonged during the admission to filter out cases of neonatal hypothermia that is non-therapeutic and not intentional.
This is a work in progress and we welcome any feedback!
Thanks @Tony_Widenor – and welcome to you and your classmates to the OHDSI forums!
I’ve been lurking in the background working on some aspects of this definition with @Khyzer_Aziz when we’re able to connect, anticipating when we’re not, and essentially running a mini-reproducibility study
In working through some aspects of what your group is proposing, I’ll share some learnings, implementations, and suggest some next steps in Cohort Diagnostics.
Proceeding along the different cohort entry pathways in your figure:
Inpatient age <0.02. I was uncertain about the impact of a decimal age value, not knowing how well the decimal value would play with different databases. Attrition wasn’t bad across a few databases I looked at. It would likely do a good job in catching our desired index admission (instead of some other pediatric admission, with holdover HIE codes, with age < 1. Great pick up! I still worry a little bit, but agree it’s worth a try and use it going forward.
Explicit HIE condition pathway. For reasons expressed before, we expect HIE to be very specific. HIE is a standard concept in the OHDSI vocabulary. From exploring parent concepts, and from reviewing some timelines, I’d also suggest that ‘Perinatal Anoxic ischemic Brain Injury’ looks to be effectively used as a synonym; It’s not a child of HIE or otherwise mapped to HIE in our ontology but I’d be curious for some expert thougths on whether such mapping should exist. If so, and if our experiments offer further evidence that are effectively synonyms, We can offer that suggestion to the vocabulary team, the broader vocabulary neighbourhood might benefit from another look.
a. I’d suggest we can examine / ‘prove out’ or examine the specificity of these (and induction of hypothermia, below) by comparing to other (presumably quite specific) combinations in cohort Diagnostics - I’ll outline that in the next post.
Suspected HIE from related condition pathway
a. Defining ‘related condition’
i. One possibility is to walk up the vocabulary hierarchy from HIE. Another lineage descends from ‘Brain Damage due to Hypoxia’ that has many concepts that are semantically similar to HIE. Long story short – I found that counts there were loaded into ‘Perinatal Anoxic Ischemic Brain Injury’, and it didn’t seem to offer much in the way of marginal gain; and those concepts are otherwise also represented in ‘encephalopathy’ below.
ii. A second possibility is a broader notion of ‘encephalopathy’, that might be in keeping with being caused by HIE. To do this, I iterated in our PHOEBE recommender system. Dr. Aziz and I also compared some notes. Interestingly and a hat tip to @aostropolets , PHOEBE also suggested concepts relating to low apgar scores (that you note in your diagram, which is kind of neat). The counts are low, but I expanded on those and included them in an act of PHOEBE worship.
iii. Combination of Additional potentially confirming data pathway
I examined a few of these procedures. I understand there’s a desire to impose constraints on the time line to reflect a typical HIE trajectory. (i.e. there was interest in echo within 3d, brain MRI after 5d, possibly echoencephalography (expanded to brain US) within 3d etc).
MRI caused considerable attrition, and may also be worth discussing the impact of a future event in a cohort entry criteria
Measurements may impact how well the definition generalizes to other datasets, and are alot of work (figuring out units, etc).
Went forward with echo (I note it’s relatively narrowly defined), and I went with ‘brain ultrasonography’ as (a parent of echoencephalography), within 3d of index.
Suspected HIE from Related treatment pathway
a. Explicit therapeutic hypothermia procedure pathway. ‘Induction of hypothermia’ seems reasonably specific for HIE in claims based data sources I looked at, but poorly captured (i.e. appears to be in 10-20% of HIE records). Because of that, we could include it in our experimentation around ‘specific’ HIE codes (ie. is it specific enough, to simply allow cohort entry?).
i. In other data sources (e.g. Stanford) , I do see it show up in cardiac surgery patients, which likely reflects its use in bypass / on pump procedures… so it may very well be reasonable to ask for additional evidence along that entry pathway.
b. Suspected therapeutic Hypothermia from Temp ≤34.5 (I asserted a requirement of 4 occurrences for ‘sustained’ here).
i. Zero hits in claims sources, not a surprise.
ii. Interestingly seems to pull out a lot of pediatric cardiac surgery patients in Stanford.
This makes me wonder if the Stanford ETL has temperature data from anesthetic records, but perhaps not NICU records, or perhaps just ones that are dredged up by my guess as to how temperature is recorded. If so, this could illustrate how a data element that improves performance at one site (JHU), might degrade it at another (Stanford).
iii. Some characterization and timeline review experiments also revealed ‘condition occurrences’ of hypothermia, might be getting used as a surrogate, as were codes relating to the ‘treatment of hypothermia’ (in ICD10 (I can’t identify an ICD10 PCS code for induction of hypothermia with some quick searching - which may relate to our observation above?). I’ve included all of these ideas in a Union representing ‘some other representation of hypothermia’, shown in the figure below.
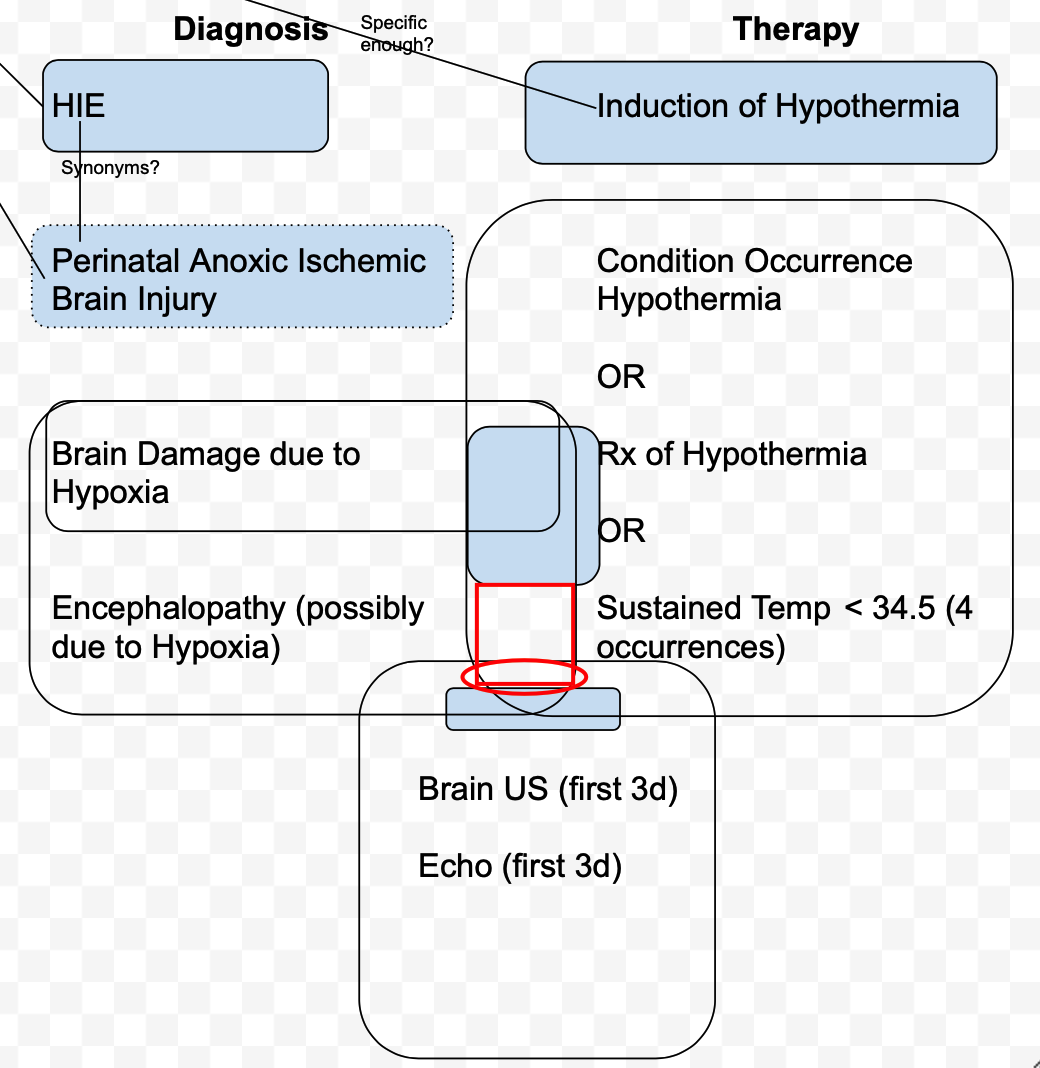
I’ve put together a diagram that illustrates how some of these ideas could be empirically tested in CohortDiagnostics.
I’ve arranged things (very roughly) along an axis of (presumed) specificity, and across 2 main domains of inquiry that we’re pursuing: concepts pertaining to Diagnosis, and Therapy.
I’ll post more about what we can try there shortly.
@Christian_Reich and others have advocated that we should be proving out whether increasing the complexity of a cohort definition is adding value.
I took an approach where (I hope) we can examine that to some extent by looking at combinatorics of components, and the marginal value brought by the contribution of a new component.
Simply stated however: It’s not a tractable human activity to test all possible combinatorics / components / variations.
So if we’re going to phenotype with our current tools, we still need to make some simplifying assumptions (in particular, reflected by the groupings we’ve made). But there is quite possibly an adjacent phenotyping field here; it taps into previous comments I know I’ve heard from @Adam_Black , for instance, around leveraging CohortAlgebra to do something similar.
Within cohort diagnostics, I’d suggest we
Establish a ‘base case’ of patients who we suspect have HIE by looking at some (presumably high specificity) component combinations. We can prove the specificity with timeline review if there are doubters.
It is otherwise hard to get a sense as to ‘is this good enough?’ or ‘how close is this to what I expect?’, in population level validation.
We can examine our hypothesis that single occurrences of the HIE, Perinatal Anoxic Ischemic Brain Injury codes, or the Induction of Hypothermia code, should be sufficient for entry to the cohort at a population level.
e.g. if ‘Induction of Hypothermia’ does look specific enough, perhaps it doesn’t require additional evidence you’ve indicated in your figure.
For our combination components, I’ve created component cohorts, as well as ‘marginal’ cohorts.
a. The idea there, is that we’ll look to explicitly examine the component as well as the additional, marginal contribution of patients to the cohort, that wouldn’t have already been included through the more specific codes.
b. The component contribution could be considered the intersect of, for e.g. Encephalopathy + (Hypothermia concepts) shown in the diagram.
c. The marginal contribution would be those intersects minus the shaded blue area within the intersect, that would have already been captured by the ‘blue’ concepts (areas approximate, of course). For e.g. as noted above, using a parent of ‘Brain damage due to Hypoxia’ was found to be quite small (<10% by memory) when ‘Perinatal Anoxic Ischemic Brain Injury’ was removed; so we’ll only consider the marginal contribution from the broader ‘Encephalopathy’ concept set.
Finally, I’ve put together some candidate cohort definitions, likely complete with logical errors . Not knowing the result of our experiments, they may be premature, but I suspect based on tests / development thus far we’ll be able to land on one of them.
The cohorts are in demo atlas. Big thanks to @Gowtham_Rao for porting them over there due to some technical issues I’m having, and running CohortDiagnostics in Family time.
Many in demo Atlas represent work in progress, were moved over – apologies for the clutter).
The ones of interest to our cohort diagnostics run (cohort ids accurate, names are not):
High specificity components
HIE x 2: 1781956
HIE AND Induction: 1781968
(HIE or Perinatal Anoxic BI) x2 :1781973
(HIE OR Perinatal Anoxic BI) AND Induction: 1781968
Single concept set components
HIE 1781960
Perinatal Anoxic BI: 1781957
Induction of Hypothermia: 1781958
Thanks @Gowtham_Rao , for the cohort diagnostics results.
Assessing individual Components
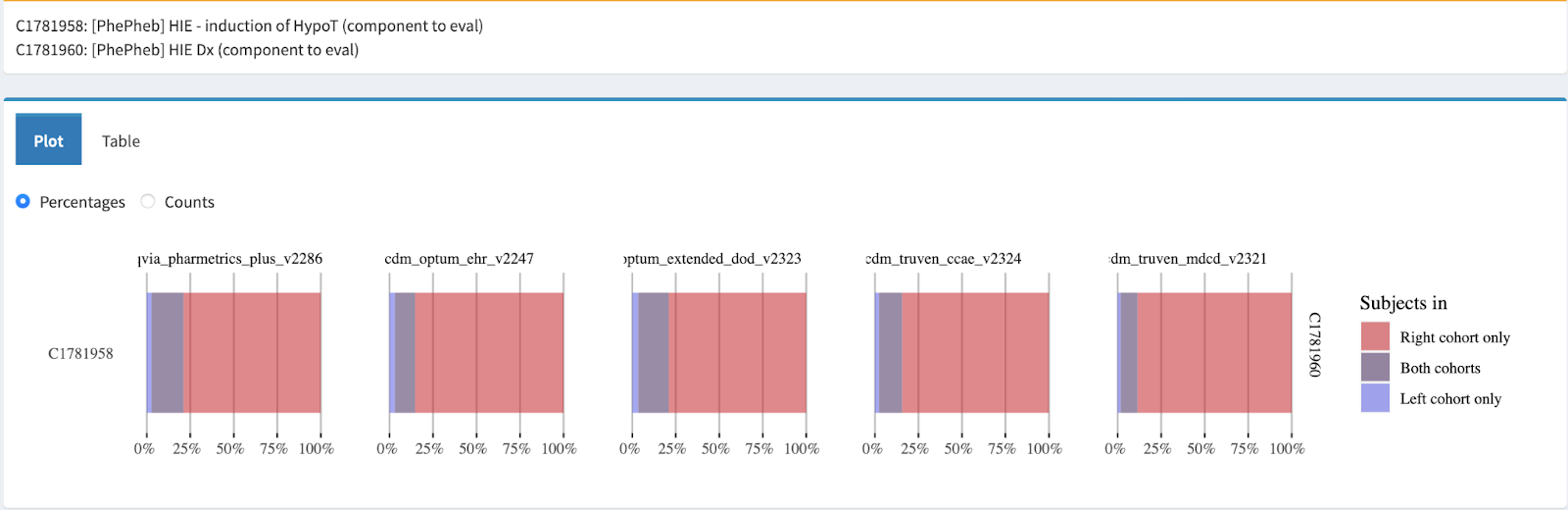
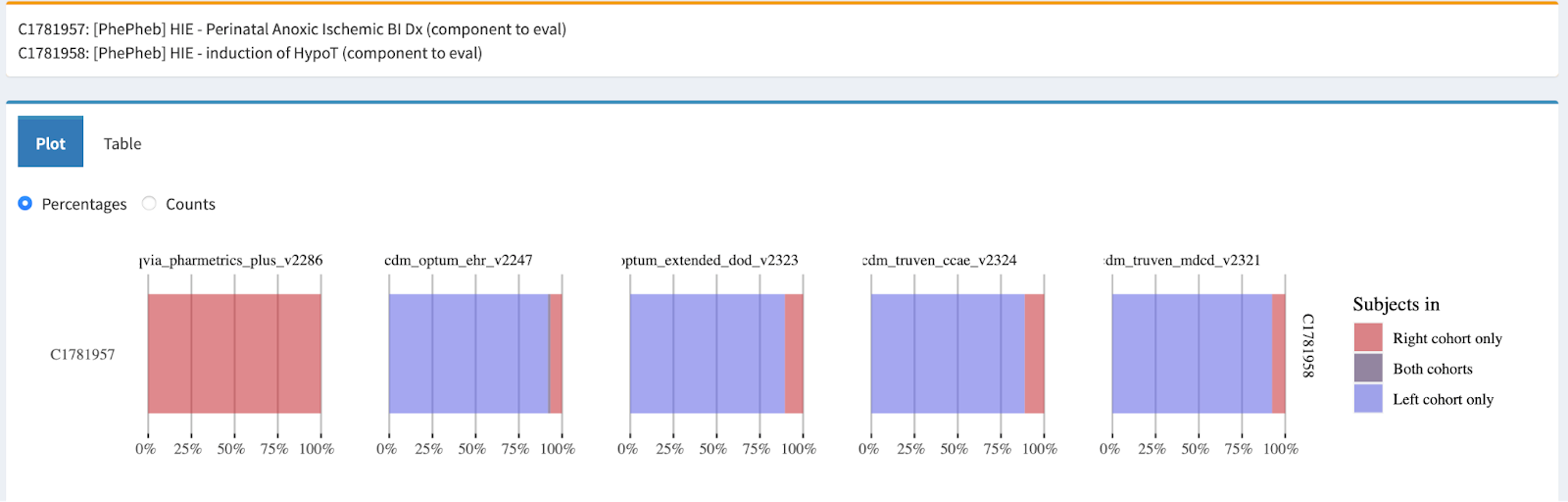
We can get a sense of how those ‘single concept entry’ concepts are distributed across the cohort diagnostics data sources by looking at cohort overlap between them.
Each individual ‘single concept’ component, overlapped with a union of all three; bottom row shows that union cohort (right), individual constituents (left cohorts).
Bottom row shows that induction of hypo T (958) is a lesser contributor, as we noted.
Pharmetrics is loaded on HIE, others more of a mix. Data sources likely tend to use one or the other, with the exception of Optum EHR) (middle row, 957 vs 960).
Reasonable split between HIE and PAIBI otherwise, so we may want both if they are both reasonably specific.
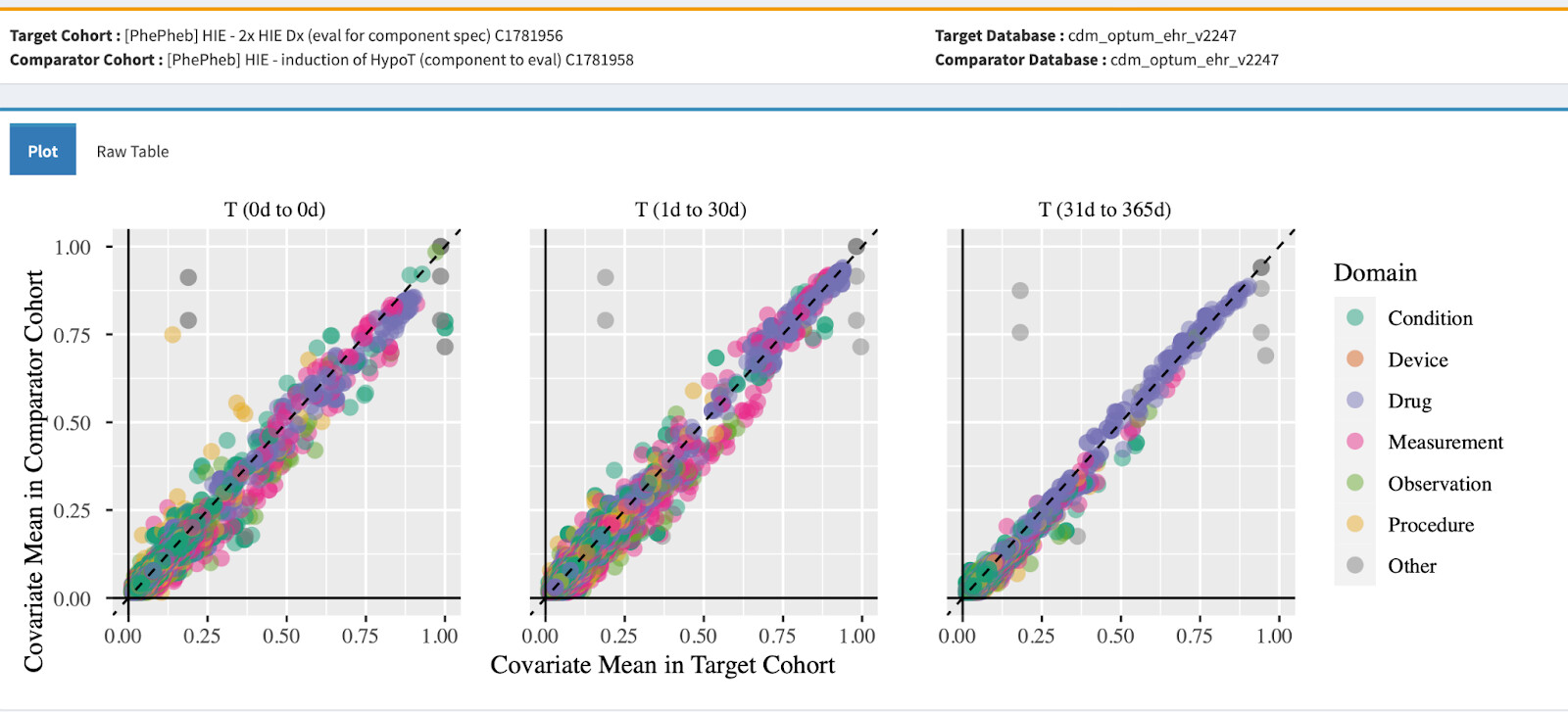
Looking at overlap of ‘Induction of Hypothermia’ and HIE:
Given the degree of overlap between Induction and HIE, the covariate plot below is not surprising. Shown here for Optum EHR,which had the most heterogenatiety in terms of PAIBI vs HIE use, and the smallest overlap of HIE and Induction (although most Induction is still also HIE). Comparing one of our ‘specific’ components (HIE x2) and Induction:
A reasonable argument could be made here, that we should be comparing HIE and the marginal contribution of Induction of Hypothermia (i.e. Induction AND NOT (HIE or PAIBI). We can do that. But based on the overlap so far, I’m pretty encouraged at Induction being a candidate to permit cohort entry (worth recalling that all these statements are conditioned on the other cohort criteria, in particular age <0.02).
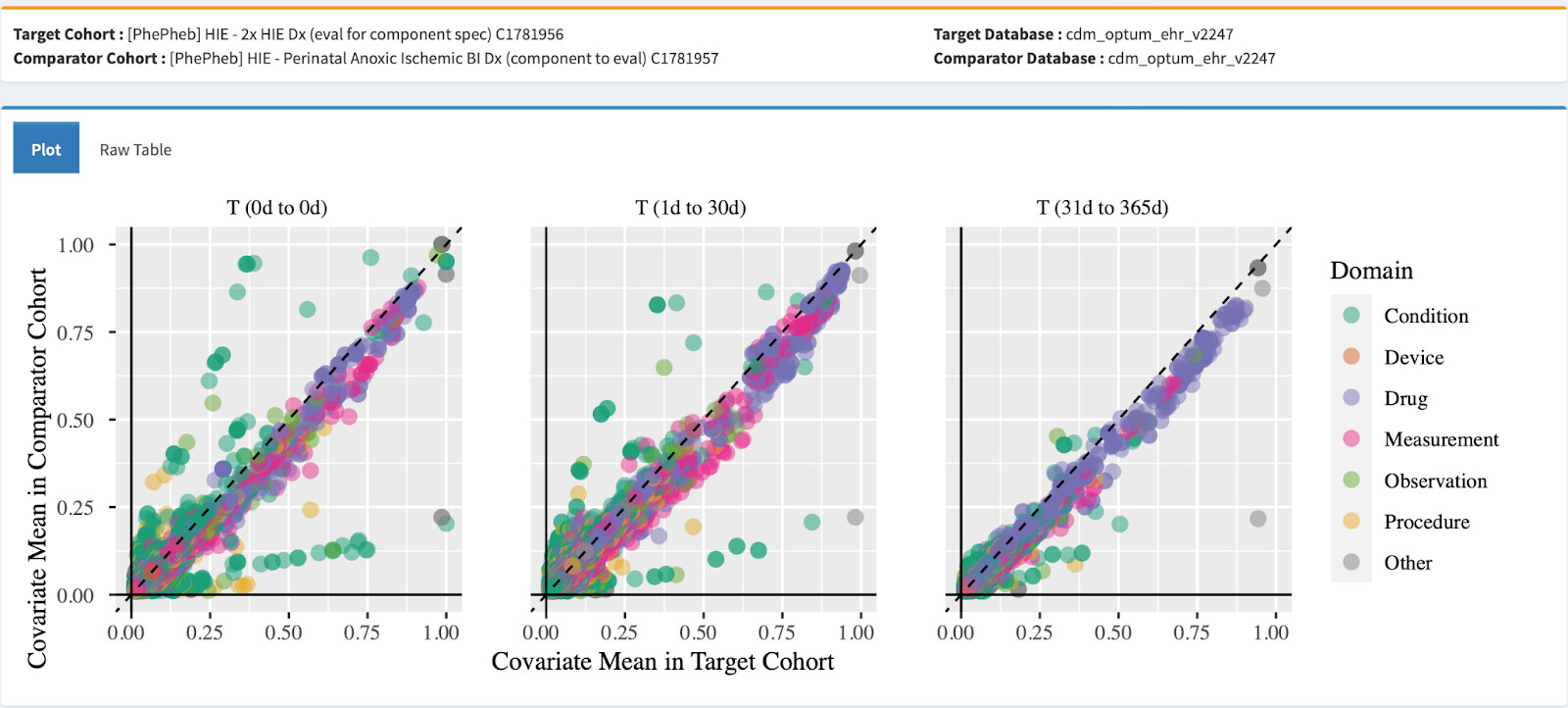
Some off diagonal elements - many are conditions that reflect the ontology hierarchy. But there is some mass in the lower left corner above the diagonal, with clusters there that pertain to Apnea, sepsis, and respiratory collapse. That makes me wonder about a specificity issue with Perinatal anoxic ischemic BI, in that it may also be applied to anoxic BI caused by circulatory collapse. (Could also consider survivor bias in requiring 2 HIE codes in 30 d - but the plot between single occurrence of HIE and Anox BI look similar). Looking at cohort characterization, resp failure in PAIBI is prevalent (40-50%), but it is also reasonably prevalent in the HIE cohort (20-40%).
In terms of prevalence of the mainstay / specific therapy - Induction of hypothermia is 16-23% in the PAIBI, 8-14% in HIE, 14-20% in (HIE x2).
So I’d be reasonably comfortable having any of HIE, Perinatal Anoxic Ischemic Brain Injury, or Induction of hypothermia qualify for cohort entry.
Based on that, I’d suggest 1781966 ([PhePheb] HIE - HIE Dx OR Perinatal Anox-Isch BI Dx OR induction of HypoT (eval as candidate)) is a baseline candidate.
Assessing combination components
First - what is the additional contribution, with regard to numbers, of the combination components?
The plot here is for CCAE (only one available right now as Cohort Diagnostics refreshes); but results across other databases were similar when I reviewed them last night. For all that work, we gain approx 8-10% (HIE Dx OR Peri ABI OR induction of HypoT OR (Enceph AND HypoT) or 4-6% (HIE Dx OR Peri ABI OR induct HypoT OR (Encep AND HypoT AND Proc).
We can look at those populations directly with our marginal cohorts.
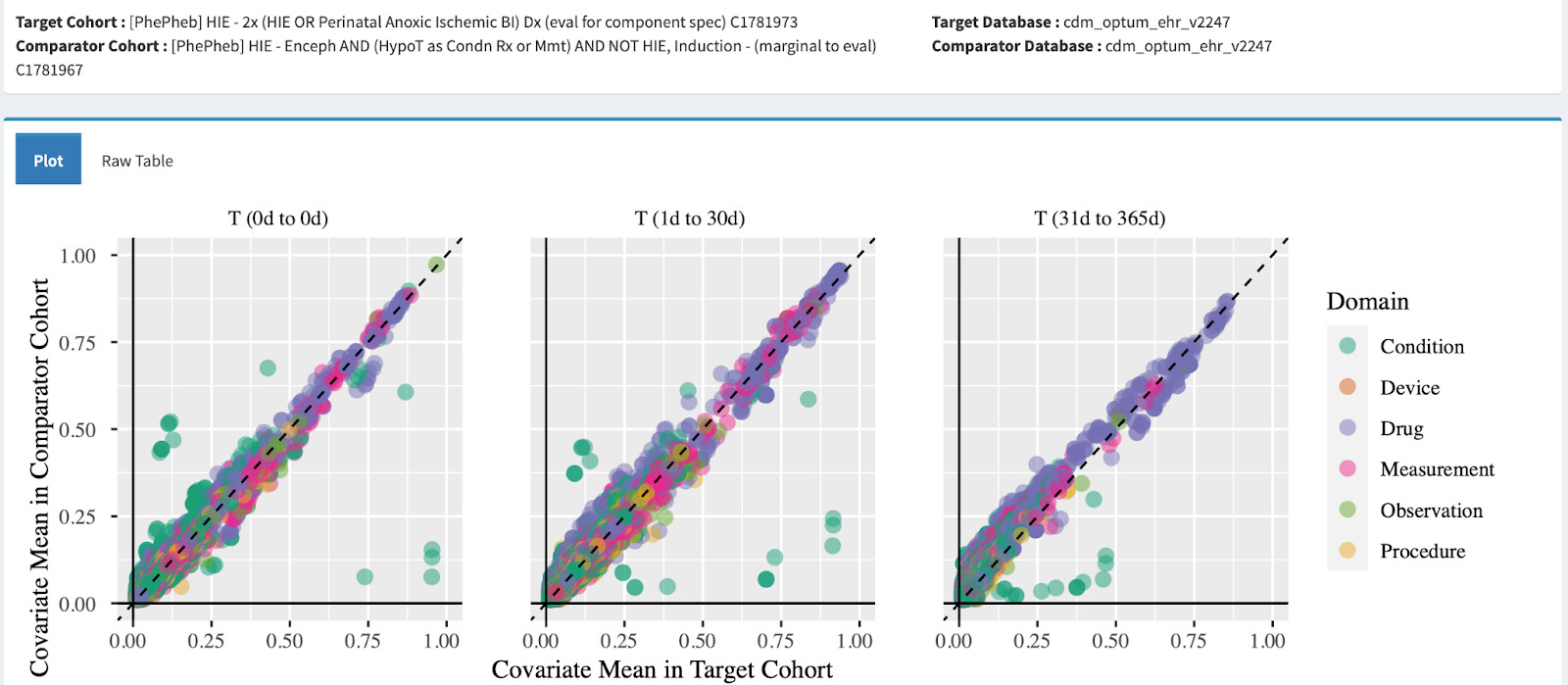
This comparison against 2x(HIE or Perinatal Anoxic Ischemic BI) looks like there’s reasonable covariate alignment. It may not be the same story across all databases:
[PhePheb] HIE - Enceph AND (HypoT as Cdn OR Rx OR Mmt) AND (Echo + Een) AND NOT (HIE, ABI, Induct)
I.e. red circle above
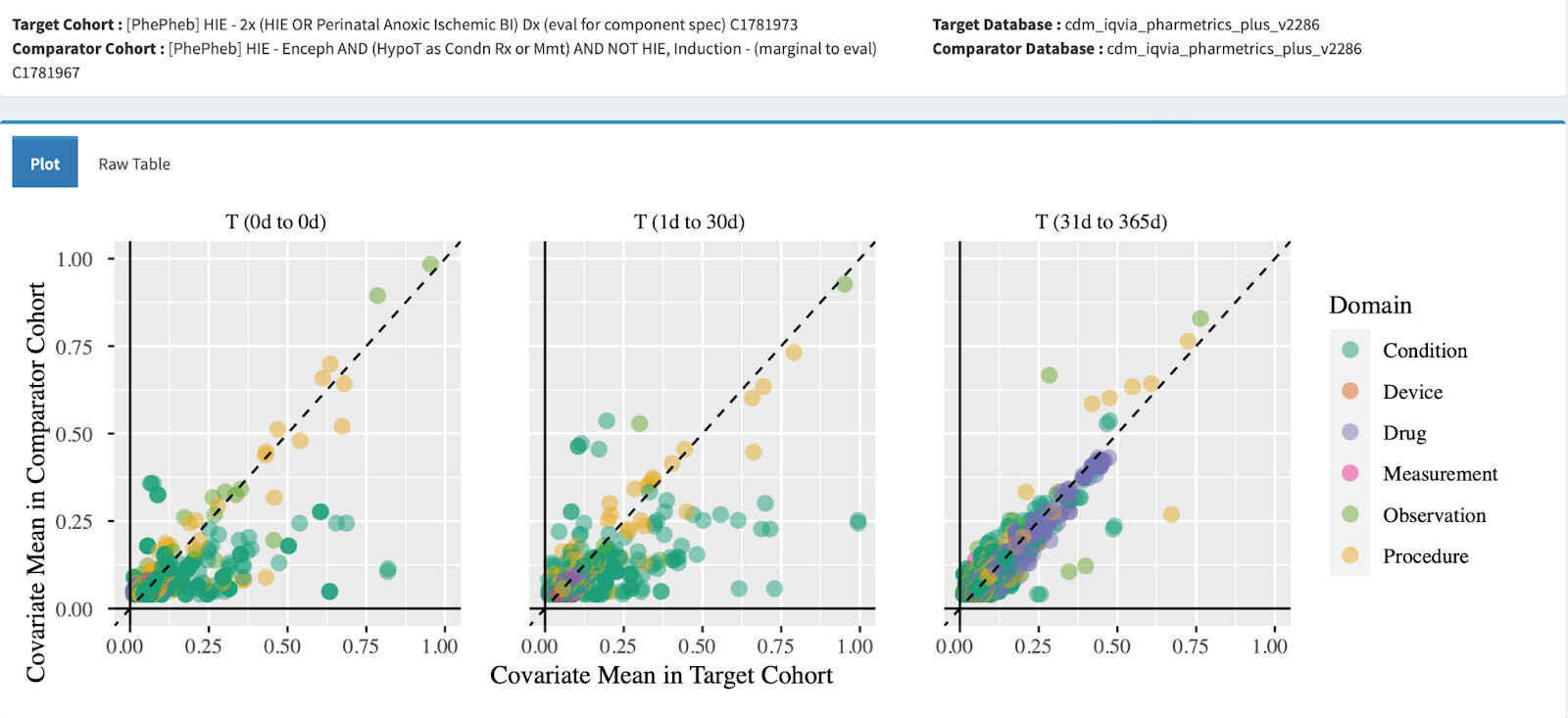
Interestingly, while you’d think we’d see even further alignment with a (presumably more specific) combination cohort that also included procedure codes, we see this:
There’s a significant off diagonal contribution here, things look worse in other data sources. In looking into it, it’s a bit hard to sort out what might be going on. There are more ‘critical care things’ happening in the marginal. There also seems to be more heart disease / congenital heart defects. It may simply be that the criteria draws out critical care trajectories / trajectories with densities that satisfy the procedure criteria (and perhaps that’s why it seems like there’s a vertical translation of the line).
Edit: there’s an additional oddity with the complete absence of ‘Coveriate Mean in Comparator’ of <0.125; so will have to examine this too - perhaps there’s different reason the plot looks translated.
Regardless, I would hesitate to include them without further characterization / evidence.
I can also offer that in another EMR source (stanford) the marginal contribution from this criteria (otherwise a cohort of >400) is less than 10.
In sum, I would propose:
We consider 1781966 [PhePheb] HIE - HIE Dx OR Perinatal Anox-Isch BI Dx OR induction of HypoT (eval as candidate) as a candidate for the library
In conjunction with the reviewer, we undertake additional investigation (e.g time line review ) of the ‘combination cohort’ marginals, to better understand their contribution
a) Near term could consider a cohort iteration that includes Enceph AND (HypoT as Condn Rx or Mmt)
b) Would explore procedure criteria further before inclusion so that we understand the impact in our network of data sources.
c) We could even consider comparison of our marginals to pheValuator results, which could tell us explicitly what their TN/FN contribution (based on that probabilistic reference standard) would be in that data source.


 . Not knowing the result of our experiments, they may be premature, but I suspect based on tests / development thus far we’ll be able to land on one of them.
. Not knowing the result of our experiments, they may be premature, but I suspect based on tests / development thus far we’ll be able to land on one of them.