This is a complex clinical idea - and i have found conflicting ways in authoritative sources have defined it. This makes it difficult to phenotype. Can we phenotype Cardiomyopathy? A general principle that we follow - If we cannot come to shared understanding of what the phenotype is - by authoring a clear clinical description - then we probably cannot phenotype it?
I started by reviewing authoritative sources (Harrison’s text book, Uptodate) and put my notes here. Because of the wide variation, i struggled because the sub-types were truly different clinical ideas and considering them as one broad “cardiomyopathy” seemed not appropriate.
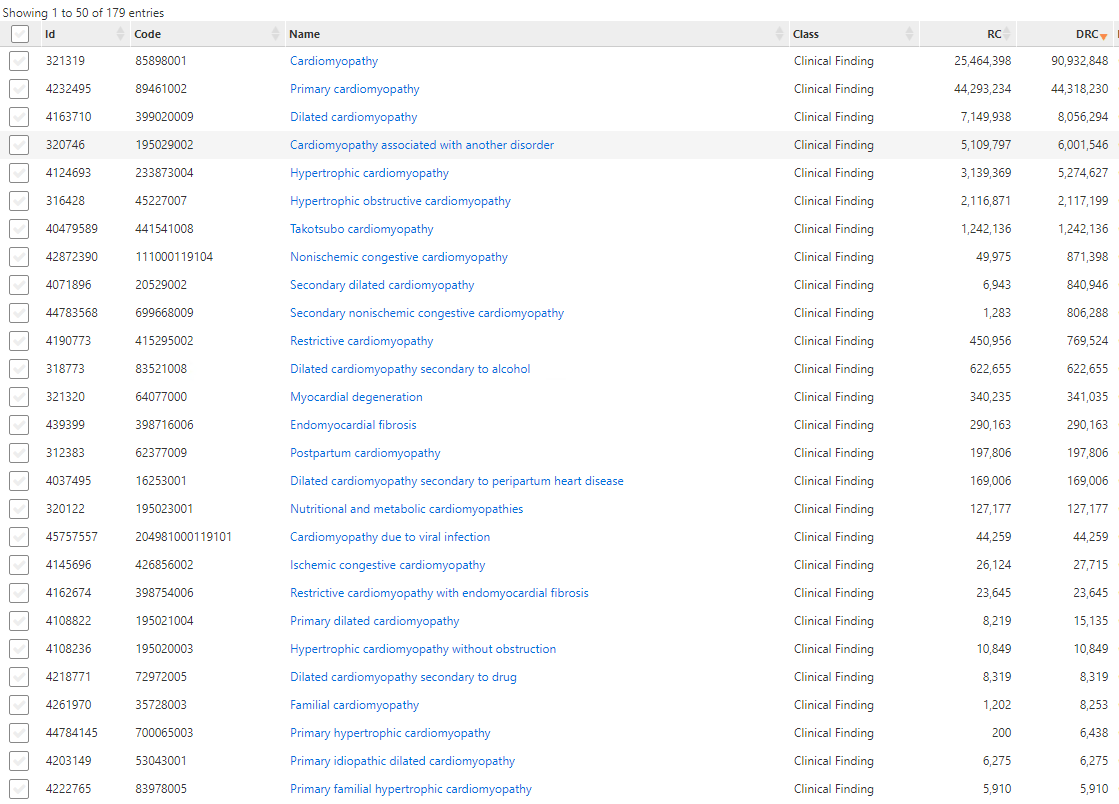
Because i felt like i was stuck - i went to Atlas and did a lexical search and found that there were many concept id’s for the idea of cardiomyopathy with two of them accounting for almost all of the concept id. These two were also non specific - and different from the contemporary classification of dilated cardiomyopathy, restrictive cardiomyopathy and hypertrophic cardiomyopathy.
I then investigated the trends in use of such codes in various data sources. see ARES reports for concept id and found that their utilization changed (increased dramatically) after 2016 (in US datasets) when the switch happened from ICD9-CM to ICD10-CM.
After thought - i decided to make five different cohort definitions/phenotypes and evaluate them
Cardiomyopathy (broad - includes all sub types including cardiomyopathy with known cardiac causes like ischemia) described here - this may be expected to have the highest sensitivity but lowest specificity.
Cardiomyopathy (without known cardiac causes prior to index date) - this maybe considered less sensitivity and more specificity compared to 1
contemporary definition for cardiomyopathy is a myocardial disorder in which the heart muscle is structurally and functionally abnormal in the absence of coronary artery disease, hypertension, valvular disease, and congenital heart disease sufficient to explain the observed myocardial abnormality.
In clinical practice, however, the term “cardiomyopathy” has also been applied to diseases of known cardiovascular cause (eg, “ischemic cardiomyopathy” and “hypertensive cardiomyopathy”).
A 2006 AHA scientific statement proposed a contemporary definition and classification of the cardiomyopathies [4]. The expert consensus panel proposed the following definition: “Cardiomyopathies are a heterogeneous group of diseases of the myocardium associated with mechanical and/or electrical dysfunction that usually (but not invariably) exhibit inappropriate ventricular hypertrophy or dilation and are due to a variety of causes that frequently are genetic. Cardiomyopathies either are confined to the heart or are a part of generalized systemic disorders, often leading to cardiovascular death or progressive heart failure-related disability.”
Overview: Primary disease of heart muscle. Three major cardiomyopathy each with different presentation and management plan. They are considered a different disease - although all are disease of heart muscle.
Dilated Cardiomyopathy has poor systolic contractile function (may effect both ventricles)
Restrictive Cardiomyopathy has abnormal diastolic relaxation (infiltrative disease e.g. amyloidosis, sarcoidosis), storage disease, fibrotic disorders
Hypertrophic Cardiomyopathy: marked LV hypertrophy without hypertension or valvular disease.
Presentation: Varies by type - Exercise intolerance, arrythmia, cardiac failure, valvular regurgitation. Many maybe asymptomatic in beginning.
Assessment: Search for the cause. may need cardiac biopsy, genetic testing, cardiac catheterization.
Plan: Treat the cause (immunosuppression) ; manage the symptoms (e.g. manage heart failure); maybe candidates for cardiac transplantation.
Differential diagnosis: heart failure, restrictive cardiomyopathy, myocarditis
The top two concept id that accounts for ~70,000 records (25,464,398 + 44,293,234) of about 90,000 records total - are non specific to the various major sub-types of cardiomyopathy. This is an indication that it is most probably not possible, in observational data - to discern between the major subtypes of dilated cardiomyopathy, hypertrophic cardiomyopathy and restrictive cardiomyopathy.
Then there are items in the search - that sound like Cardiomyopathy - but are not? e.g. is
Takotsubo cardiomyopathy a type of cardiomyopathy? Or is it a misnomer for a temporary condition.
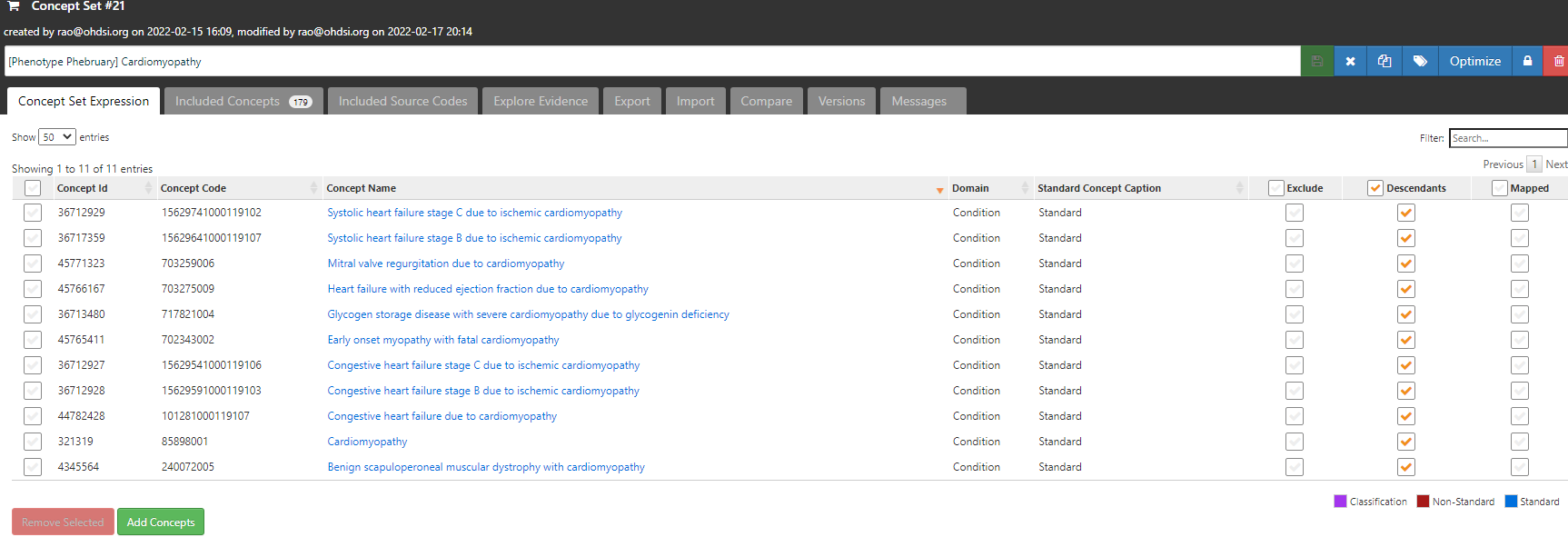
Creation of concept set expression
I could do a concept set expression like this concept set 21 but i dont think thats right because i dont have a clinical description.
Any clinicians/cardiologists in OHDSI who can help me?
Should we build a cohort with the broad cardiomyopathy concept set expression like this?
Note:
ventricular dilation with systolic dysfunction (commonly called “ischemic cardiomyopathy” or “valvular cardiomyopathy,” although these are not defined as cardiomyopathies under current American Heart Association/European Society of Cardiology [AHA/ESC] classification systems
Clinical description - to supplement clinical description written here
Dilated Cardiomyopathy
Overview: characterization by cardiac dilation and impaired contraction of ventricles - systolic heart failure with population prevalence estimate of around 3.6 per 1,000. Many are clinically unrecognized. viruses and gene mutations are most common causes
Presentation: many asymptomatic. presents with symptoms of systolic heart failures
Assessment:
Not yet there, but the explanation of your process of phenotype development is enlightening. I am not a clinician, but looks like we will need three “full” phenotypes for each subtype with their own clinical definition process, literature review, etc. Just like different types of diabetes.
Didn’t mean it as a critic , on the contrary I am impressed by the amount of work and how thoroughly you tackle all these complex phenotypes. Let me know if I can help you further in any way.
I am not a clinician, so I’m not sure this is helpful, but looking at the concept record counts, it looks like >70% of the data is loaded on ‘cardiomyopathy’ and ‘primary cardiomyopathy’, which means that if we go down the path of trying to define subtypes, then we’ll need to figure out how to allocate the ‘non-specific’ cases (somewhat akin to the issue that @Adam_Black raised with TNBC on Day 19). Given that the data cannot parse the distinction, I wonder whether a clinical description that combines the subtypes together is useful.