OHDSI Home
|
Forums
|
Wiki
|
Github
OHDSI Forums
Phenotype Phebruary Day 15 - Acute Myocardial Infarction (STEMI/NSTEMI/UA/Chronic Angina)
Gowtham_Rao
(Gowtham Rao)
February 15, 2022, 10:07am
10
image
742×196 17.8 KB
image
710×320 15.9 KB
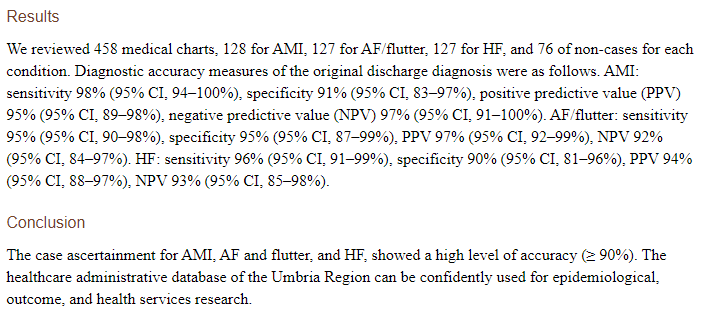
sensitivity
specificity
PPV
NPV
98% (94–100%)
91% ( 83–97%)
95% (89–98%)
97% (91–100%)
show post in topic
t