@christian - I agree that trial arms are also in scope.
I also want to document that there is communication with Columbia U on how to unify some clinical trial data conventions. (possibly to be used by the phenotypeDataExtraction package) (find similar patients given an a trial NCT)
I was discussing study data transformation with someone (think SDTM data transformed to ADAM data).
Here is another issue for the group to discuss:
To capture raw data as well as “for analysis” transformed data - I propose to use the same table (e.g., measurement) and use type columns to indicate raw vs. transformed. (just to put a proposal to the discussion)
Not capturing raw data is probably not an option. This would make OMOP inferior to current standards.
To capture transformation steps (captured in Define.XML), OMOP METADATA table could be used for that purpose.
@Vojtech_Huser - Since there were a few posters at the Symposium on using OMOP and RWE for Clinical Trial analysis, thought it might make sense to try and revive this thread.
I see a few levels of items to consider for being able to fully leverage the power of OMOP CDM with RCTs. I don’t think this is exhaustive per se, but thought it might help spur the discussion.
A: Data Model Interoperability:
CDISC SDTM conversion to OMOP CDM
CDISC ADaM conversion to OMOP CDM
OMOP conversion back to CDISC
B: RCT Administrative Records:
Patient Screening (not the recorded determination of eligibility, but that the screening took place)
Patient Randomization
C: RCT Visit Type (e.g., was the visit for screening, baseline, follow-up, etc.)
D: Non-standard Interventions and Outcomes (e.g., how to record and deal with investigational therapies, unvalidated PROs, etc.)
@Vojtech_Huser - I’m wondering where you’d recommend is the best place to capture the issues and lessons learned from our respective CDISC conversion efforts?
One community effort could be to produce “SOURCE_TO_CONCEPT” map for the lab test below: (that we saw in the sample data)
(Also tagging @Craig_Mayer in our clinical research informatics team)
(observations also pasted for those who do not click the link)
Sample data conversion results
sample CDISC data differes in format from trial RWD (3 trials)
person identifier used (SUBJID, RSUBJID,RUSUBJID))
large sample needed but not available; must also be recent (trial started and finished in the last 5 years)
SDTM manual is very long, in PDF format (this should change with CDISC SHARE initaitive)
Demographic (DM) domain does not contain year of birth. It is not clear at what time age is calculated. (at first visit of the subject?; day 1 of the trial) (convention)
trial data may be organized by visit number (not absolute date)
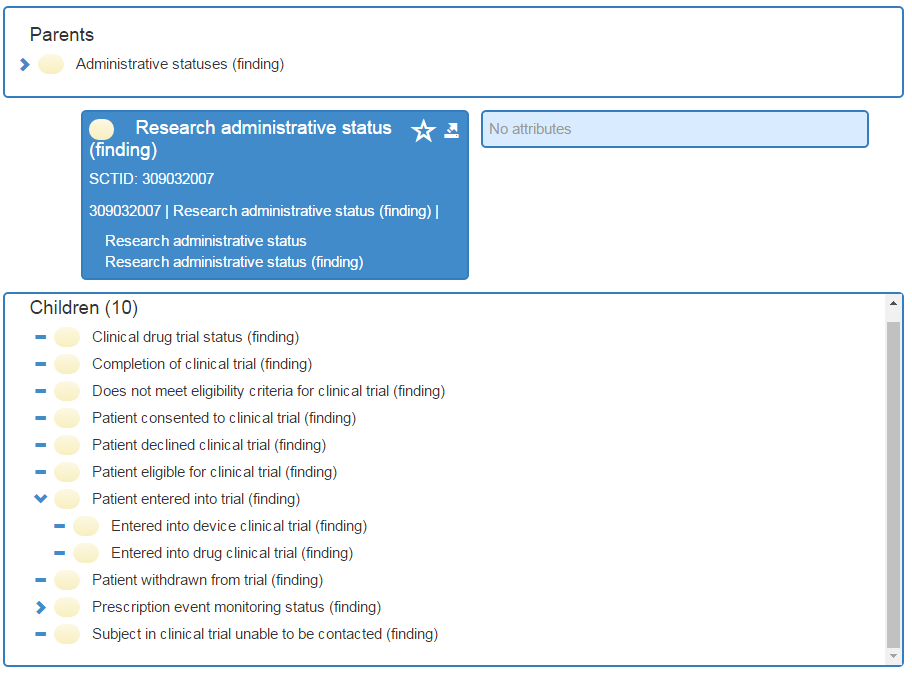
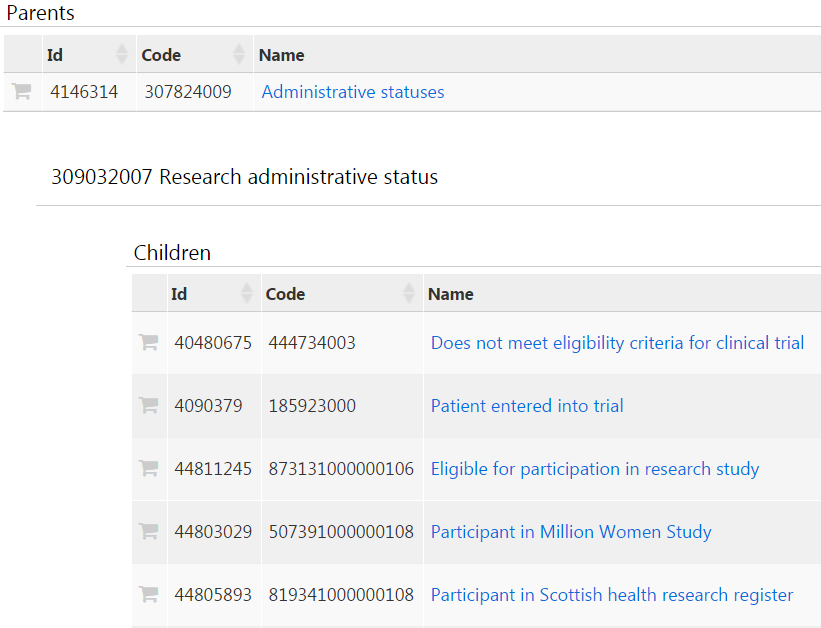
Demographic (DM) domain data on screen failure or arm: missing suitable concept_id (issue) (tentatively using LOINC 68839-0| Research Note) (todo new concept)
LOINC codes will be used in SDTM (in 2018, FDA clarified a LOINC strategy) so detailed mapping is not pursued.
Assignment into arms can be in COHORT table or as OBSERVATION or other table (convention).
Vital Signs (VS) domain is very similar to Laboratory (LB) domain. Both have standard units and original value and numeric value. LB has exact datetime, whereas VS has only date (issue).
_source_value columns were sometimes overloaded with multiple elements separated by delimiters (issue)
Medical History (MH) domain captures a condition at a given visit (date1) but
records onset date (date2). Date2 can be null (not known) (convention) (issue)
update: the trial arm term will be in SNOMED CT in Jan 2019 !
(I submitted it)
@Vojtech_Huser What is the status of this proposal? Is there an agreement on the convention within Themis?
A next step would be to also capture the details on the study in OMOP, like name, inclusion criteria and arms. A new Study domain/table might be necessary. Or has the assumption been so far that one dataset represents the data from one clinical trial?
OMOP currently captures visits. Where a patient AND provider interact.
If a patient logs into PHR or provider mails a letter to the patient, it is a one sided event. Just patient does something or just provider does something.
From patient care and research point of view (e.g., on PHR side, ability to recruit into a applicable research study via PHR), such events matter and can be important for research.
Not just for clinical research–I would imagine for some treatment programs of the public health variety, this would be important to capture (I’m thinking of things like TB and HIV, where outreach is a routine part of clinical care). I’m working with a team to develop a EMR in Eswatini that’s pretty HIV-focused, and we are looking to build out an “outreach” module because that’s a critical part of our care program that we get evaluated on.
I have read a lot of things I could find online about how to capture trial data in CDM 5.4, but I am still not sure about the final solution.
It seems here Proposal: Clinical trial data conventions for OMOP CDM · Issue #196 · OHDSI/Themis · GitHub that there is a convention, but I was not able to find it in the documentation.
If we only have data on the trial number (as a procedure), should we use “Patient consented to clinical trial, 4163733”?