the proposal has evolved to this point:
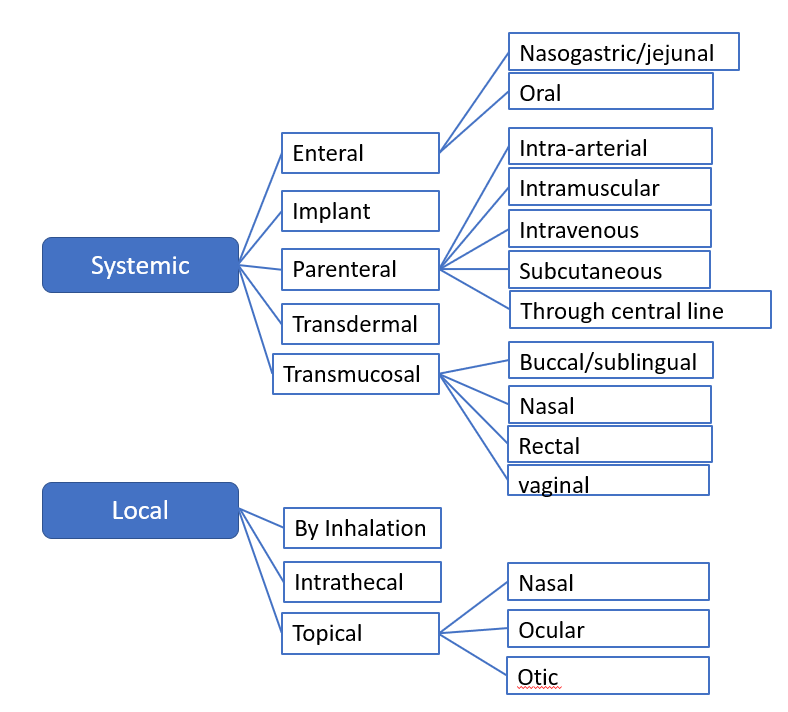
I agree with the @funaesthesia mappings.
Just to be clear, the route is a last resort. In general you would define your exposure in other ways, because you know the dose form or procedure code or whatever. Let’s keep this discussion in the way to solve the use case of estimating daily dose for systemic applications.
If people need more granularity in the local administrations, that is fine for me, but not suggested by me, because usually those does not really matter from a pharmacologic point of view.
To answer @Alexdavv point about having two nasals in the hierarchy. For me, if there is the option that something is systemic, it trumps the local application and is put in the systemic bucket, because we do not want to miss a systemic exposure, but I am happy to miss a local exposure. That being up to the ETL person is not really true, because the dose form to route mapping done by us as well decides where the drug goes (if it has a dose form).
I am not an expert in routes used by specialists (mentioned above, anaesthesia, intensive care etc.) Question is, are these theoretical questions, like nice to have, or really needed routes that you actually rely on in your research using health data?
My aim is not to solve the route problem but to have a solution that works for the time being until we have something better. We can discuss here forever, and actually never do anything ![]() I kind of see this happening when looking at the post @Alexdavv referenced Route 'standard' concepts not standard anymore? - #26 by rtmill… so it is up to you, me, all of us, that something is actually happening. Given that we are still discussing this also shows me that no one is actually using route in their data??
I kind of see this happening when looking at the post @Alexdavv referenced Route 'standard' concepts not standard anymore? - #26 by rtmill… so it is up to you, me, all of us, that something is actually happening. Given that we are still discussing this also shows me that no one is actually using route in their data??