Thanks @DTorok.
We followed this guidance when building our ETLs, but it’s clear we’re losing a lot of valuable information as we move from local concepts to OMOP standard concepts.
Here’s how we’re thinking about the flavors of ‘specialty’ for each of the tables that use these concepts:
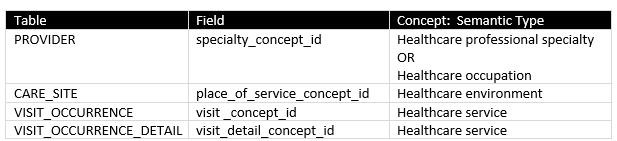
The existing vocabularies used for these concepts (NUCC, ABMS, Medicare Specialty, UB 04, CMS POS, etc.) seem well suited for the adminstrative use cases for which they were desgined, but no so much for analytics use cases (i.e., encoding and using data in an OMOP CDM).
These vocabularies are problematic for the following reasons:
- Conflation of semantic types
- Poor coverage
- Limited hierarchical relationships
- Lack of polyhierarchical relationships
- Difficulty in getting new concepts added to keep pace with needs of researchers
The discussion started by Dr. Wu here strikes me as good example of where requesting a couple of new SNOMED concepts for use in OMOP might address some of the problems identified by these researchers:
- provider_specialty_concept_id => new concept | Movement disorder neurology specialty (qualifier value) |
- place_of_service_concept_id => new concept | Movement disorder clinic (environment) |
- visit_concept_id / visit_detail_concept_id => new concept | Movement disorder services (qualifier value) |
@Christian_Reich - any historical discussions about potential for SNOMED as standard vocabulary? What are yours (and other folks’) thoughts about exploring this more rigorously?
Best,
Piper