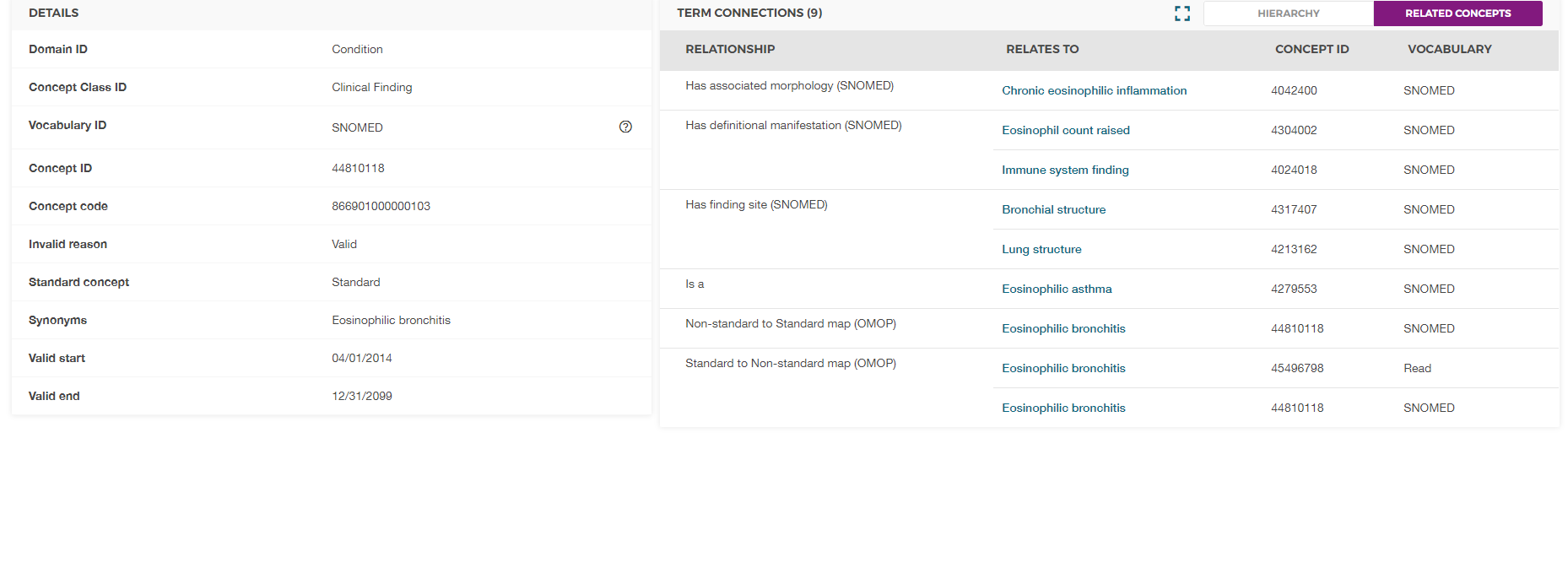
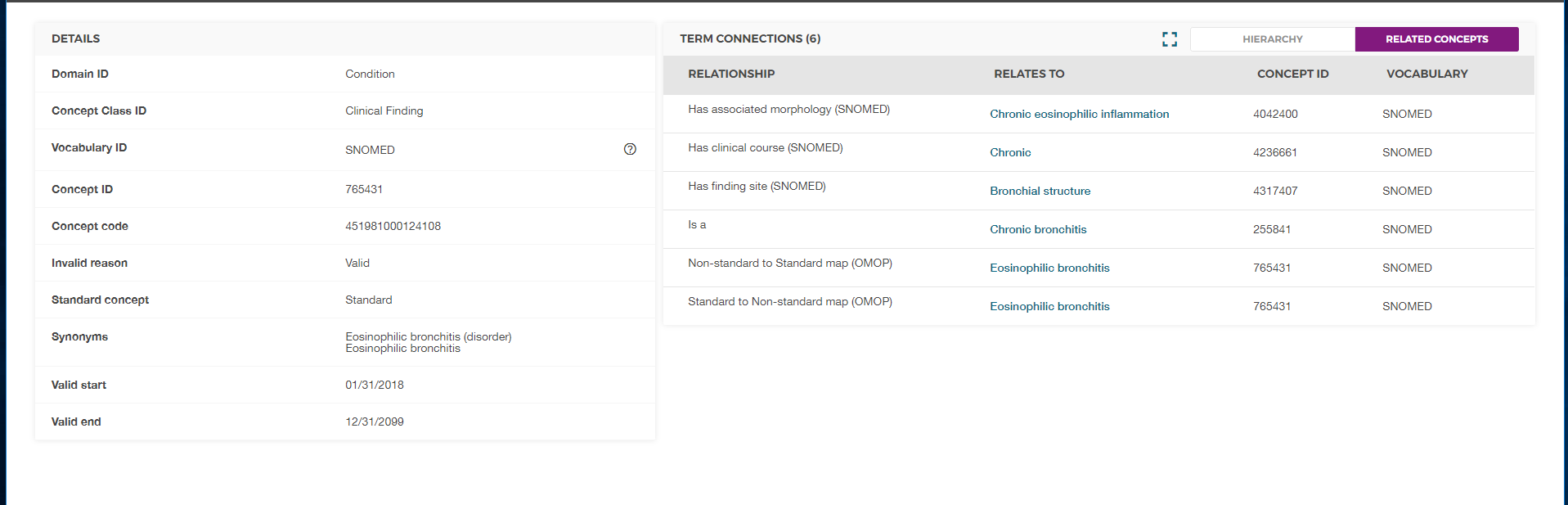
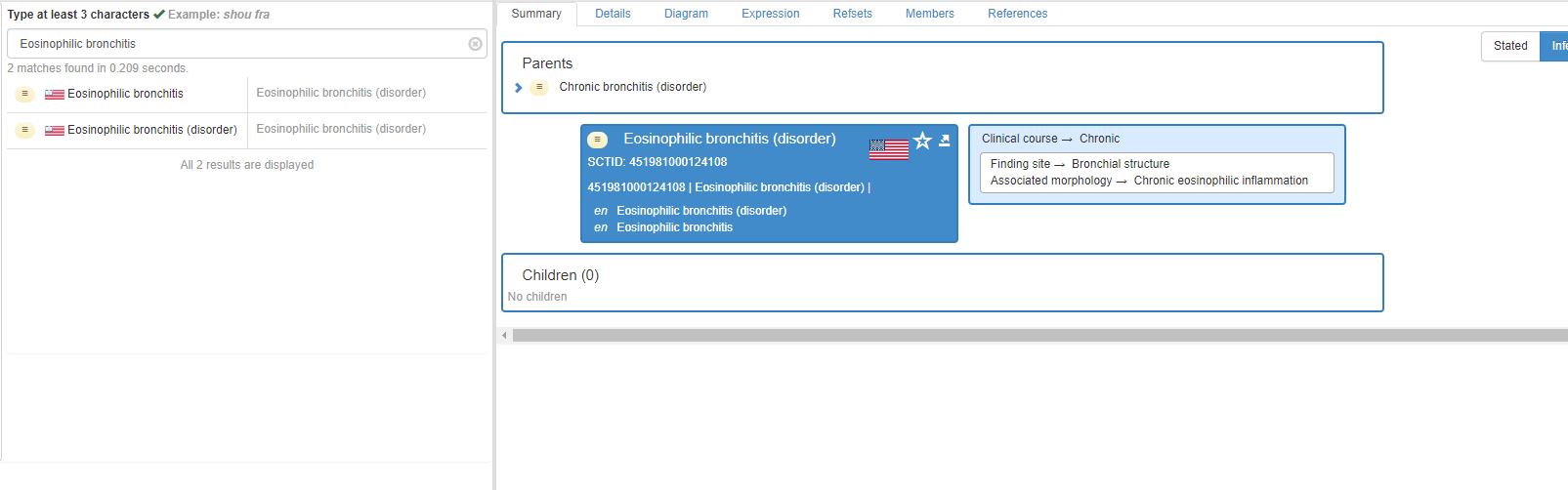
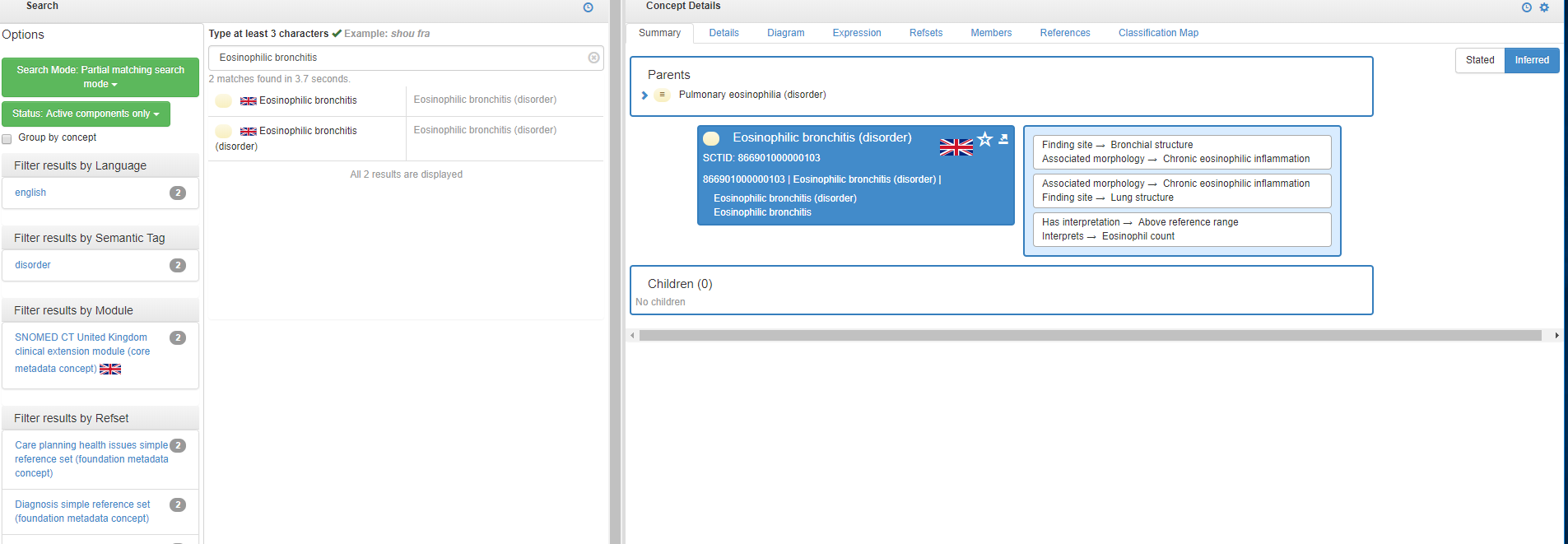
I’d say, for now, you should pick the one with a parent you think it should belong to. Here, relation to eosinophilic asthma may is more important than to chronic bronchitis, as EB has a special etiology and pathogenesis that differ from simple bronchitis.
Coming back to the general issue: I do not think that both should exists as standard. One would be mapped to another; as most of the OMOP datasets originate from US, it sounds logical to map UK SNOMED to US SNOMED. Apparently, in this case this important hierarchical feature will be lost.
So we either need to push SNOMED to fix the hierarchy where appropriate (which doesn’t seem too realistic) or investigate the discrepancies and create a mix of standard UK and US SNOMEDs (which doesn’t seem too clean).
Good analysis, indeed this comes from two extensions. Actually, I think this concept should be moved to the international release, adequately defined, and with either one of the existing concept IDs, or a new one.
One comment: It is very well possible to have this fixed by SNOMED. Submit a change request for Eosinophilic bronchitis to be added to the international release, then it will be made obsolete in the US & UK extension.
Best to reach out to your national release center to support you with that.
That’s true. Actually, @Christian_Reich has been establishing the relationships with SNOMED guys. Nevertheless, we need to look at the bigger picture: if there is one precedent, there will be more that we need to find before we send a request to SNOMED.
Yes, good to include the bigger picture. Among this is actually the question whether you want to limit to the international version of SNOMED CT or also include links to national extensions. And if the latter, whether you restrict to some extensions (e.g., UK & US) or open up to all.
If you restrict to the international release, eosinophilic bronchitis will not have a matching concept in SNOMED.