
Friends:
This is a proposal for the the long-awaited consolidation of Type Concepts. Right now, Type Concepts are organized by Domain, creating a ton of duplications, and they are a wild mixture of provenance and categorization (really “type”) indicators. Also, some of them are badly pre-coordinated and many are not intelligible if you don’t know the US reimbursement claims system.
This is a proposal to fix all that:
-
Type Concepts now really indicate provenance. We should rename them to “Provenance Concepts”, but that would be too much of a change - almost all use cases and tools would have to be refactored. So, my proposal is to bite the bullet and keep calling them “Type Concepts”.
-
All Concepts are now called in such a way that they can finish the sentence “This record was obtained from a …”. So, Concepts like “Inferred from procedure claim” is being renamed to “Claim” - they all are inferred, and there is no such a thing as a procedure claim.
-
Era 0 day persistence window records were dropped like in 2010. We don’t need that anymore.
-
Medical claims are now Inpatient, Outpatient, Facility and Professional claims. Non-medical are pharmacy, vision and dental.
-
Type concepts have a simple hierarchy. So, all of the above claims are descendants of “Claim”. The hierarchy is single-parent.
-
Instead of the 338 records we have now 63:
-
All positions on the various claims forms, which often are used to distinguish between primary (the condition the encounter is about) and the many subsequent positions go to a single “secondary” Concept in the CONDITION_STATUS_CONCEPT_ID. All death-related Type Concepts also are stripped to the actual provenance, and the death becomes a status in Condition Status; which will be released in a subsequent Forum post.
-
Condition Procedure, Primary Procedure and Secondary Procedure are not Type Concepts. They are Domain assignments.
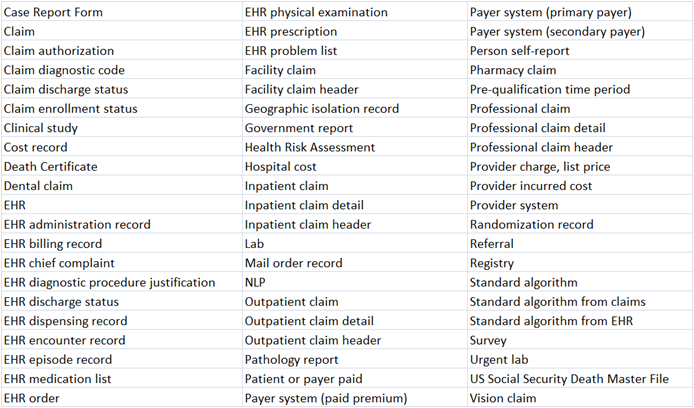
The following table shows the current Type concepts, and what they are mapped to, and their hierarchy.
Please take a look and critique.