As mentioned in our earlier update, the study Seek COVER: Development and validation of a personalized risk calculator for COVID-19 outcomes in an international network is designed to inform individual behavioral choices and help design shielding strategies during de-confinement. This has just been posted to MedRxiv, so please share this link with your respective networks!
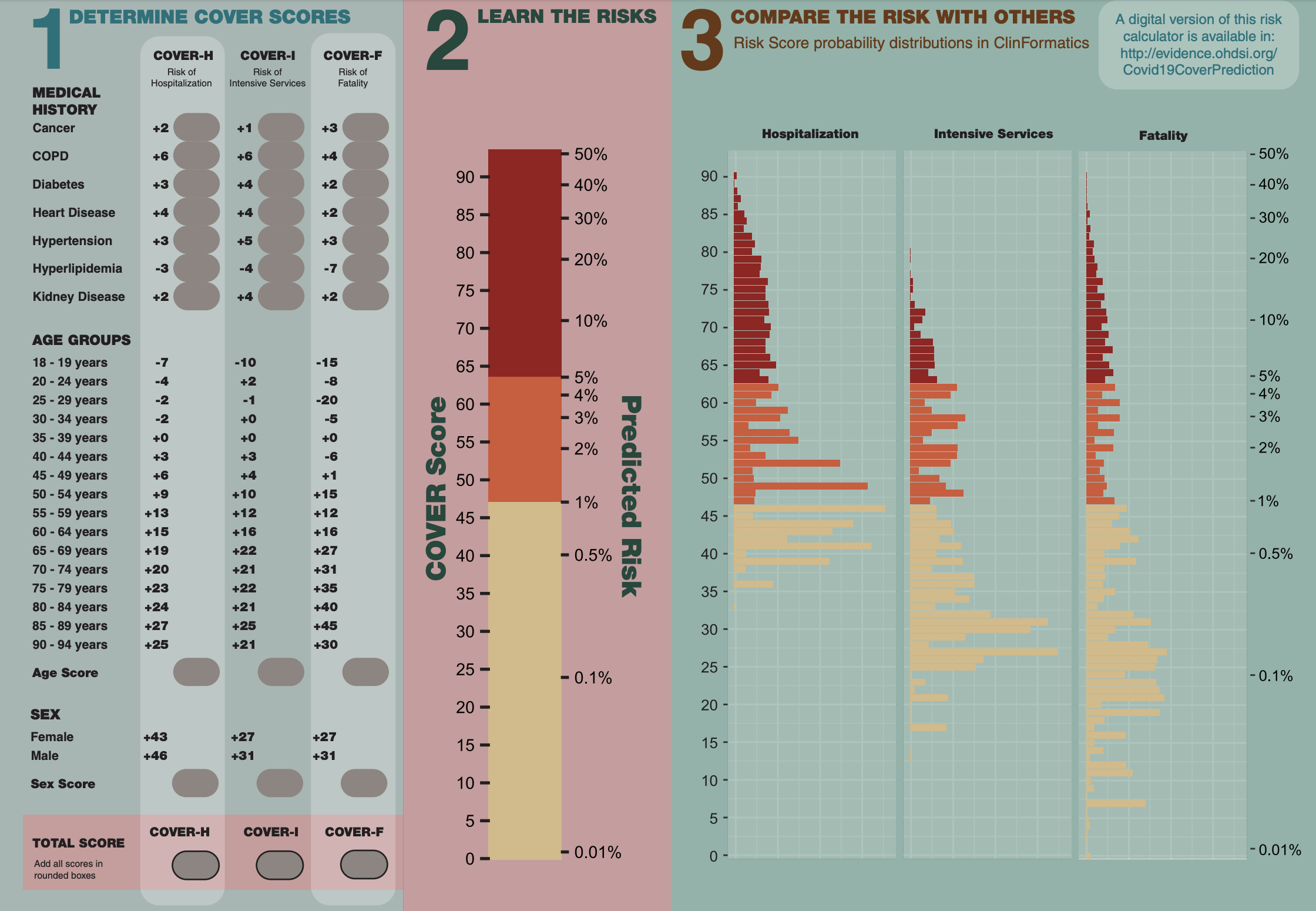
Check out the graphic below the link. As described in the study, this shows “a risk converter, which allows for easy conversion between the risk score and predicted risk of the outcomes. Furthermore, we provide a plot of the probability distribution for the three models from patients in ClinFormatics to demonstrate the expected regions the probabilities fall into. To calculate the COVER scores using Figure 1, a clinician needs to identify which predictors the patient has. The points for each of those predictors are then added to arrive at the total score. For example, if a 63-year-old female patient has diabetes and heart disease, then her risk score for hospital admission (COVER-H) is 43 (female sex) + 4 (heart disease) + 3 (diabetes) + 15 (age) = 65. The risk scores for intensive services (COVER-I) and fatality (COVER-F) are 51 and 47, respectively.”
Led by co-first authors @RossW and @aniekmarkus, the team designed a nine-predictor COVID-19 Estimated Risk (COVER) model that was validated using more than 43,000 COVID patients (following initial development and validation using more than 6.8 million patients with influenza or flu-like symptoms). This model predicts hospitalization, intensive services, and death, and can help provide reassurance for low-risk patients, while shielding high-risk patients, as many start to enter the de-confinement stage of the pandemic.
@Rijnbeek is the corresponding author, and both he and @jennareps are co-last authors. Overall there are 43 authors involved in the study, once again highlighting the global collaborative nature of the OHDSI community. Congratulations to all who were involved in this work.