Hi All,
Currently, I’m working on integration of radiology data with CDM.
While doing so, I found that RadLex was recently incorporated into LOINC. RadLex is a comprehensive lexicon of radiology terms for indexing and retrieval of radiology information resources, specifically aimed at representing clinical content associated with radiology reports.
And I found that RadLex originated code exist in OMOP concpet_ids for measurement, too.
To my knowledge, the radiology procedures are stored in Procedure_Occurrence table.
Like @Vojtech_Huser tried to standardize measurement concept_ids, we need to standardize the concept_ids for radiology procedures, too.
Actually, I don’t know how we can standardize the radiology procedures. Do you have any thought, @Christian_Reich, @Dymshyts, @gregk ?
And here goes the principal question:
how do we store the results of the MRI (and other imaging) in CDM
a) if MRI has Measurement domain?
b) if MRI has Procedure domain?
Regardless what domain (Measurement or Procedure) it comes from, I think the MRI (and other imaging) results should be first stored in Note or Note_NLP table and then use established NLP algorithm to convert them into SNOMED or ICD codes and then stored them in Condition domain with Condition_type_concept_id “NLP derived”.
@Dymshyts
Yes, you got it!
My First and fundamental question is: Where should we store the fact that the patient underwent thyroid MRI, in Measurement? in Procedure?
I’d thought that this should have been stored in Procedure.
Now, we want to standardize the radiology procedure across the world. I want to follow RSNA (Radiological Society of North America), which built RadLex to standardize these first. Then, we need to store these data into Measurement because of OMOP-CDM’s rule. That’s why I’m confused. And that’s why I want to discuss with other OHDSI members.
@QI_omop
Yes, that’s why I proposed update of the NOTE table.
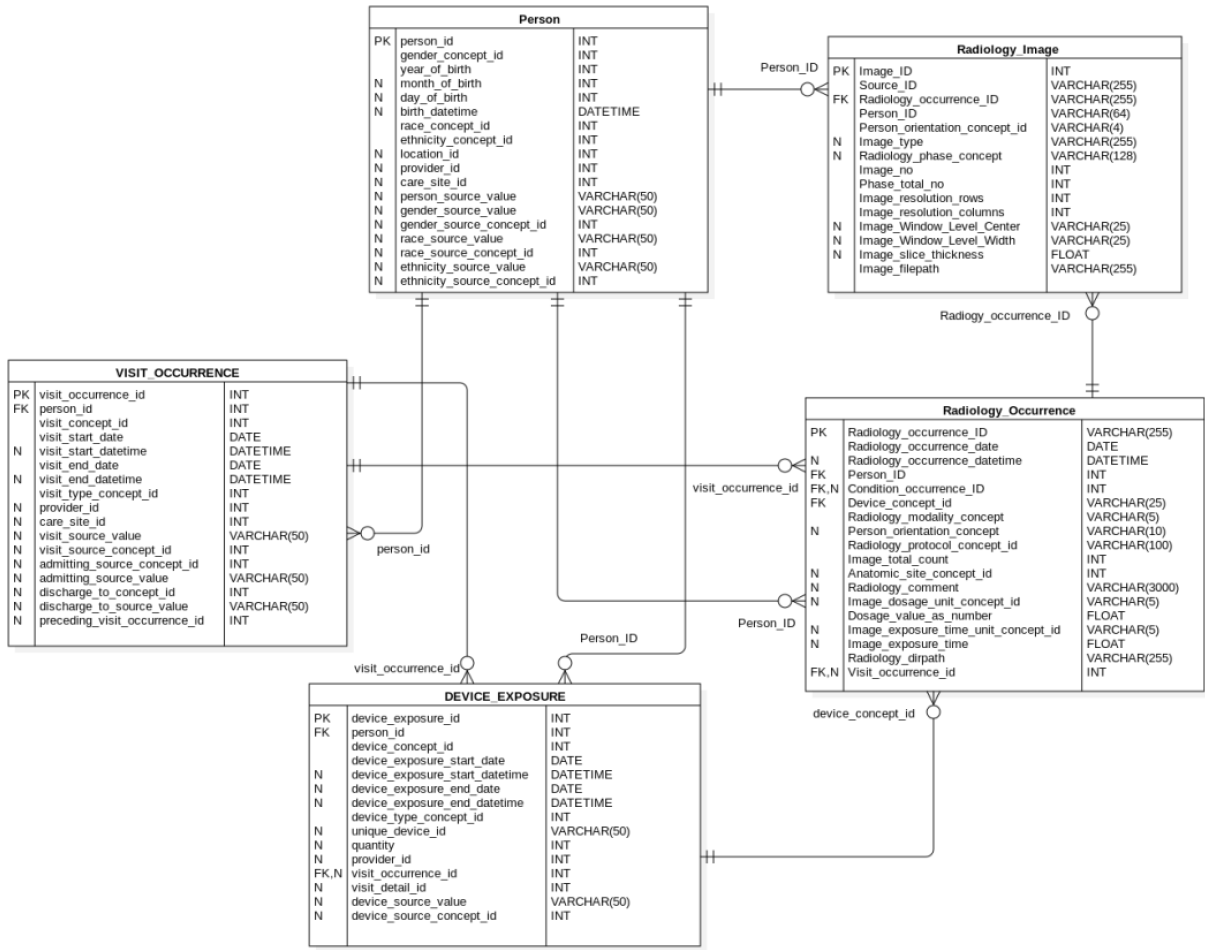
And recently, we’re developing extension model for radiology image itself, too.
It should be stored in Procedure if the result is stored in a free text (taking the SNOMED concept)
and linked through fact_relationship to the NOTE table.
And it should be stored in Measurement if the result is something exact like “Abnormal”, “Normal”, “Enlarged”, etc.
So I’m answering to my own question
Can you tell me more about the RadLex?
I 'm looking here http://www.radlex.org/, and I see much more than just the list of the concepts that I see in LOINC. For example the results of the imaging are also encoded.
In this case it sounds like a good plan:
to incorporate the imaging results from Radlex and then put them in Measurement value_as_concept_id, right?
@Christian_Reich yeah, except for the fact that this is something that goes without saying. Or, at least, it looks like that for me. Why? Because you have measurements for that and results that we can store in source_value. So why not use what vocabularies give us?
Have only procedure - put it in procedure_occurrence. Have result - can put in measurement or observation (will be SNOMED MRI abnormal or something). Observation is even better as here we aren’t talking about the exact results or parameters, but rather about an observation. Can’t parse huge NLP data - put it in Note.
I’m new to the group, am trying to get up to speed with your efforts, though I think it’s great this group is working on adding radiology to OMOP. I’d like to understand the specific use cases you have in mind for querying image data in connection with this effort. As to standardizing radiology procedures, the RadLex Playbook/LOINC effort has done that by creating a post-coordinated terminology built using RadLex atoms. See https://www.rsna.org/RadLex_Playbook.aspx.
I also want to point out that all of the key information related to images is not only in the DICOM header; the Annotation and Image Markup project (AIM) created a data model for image data, and this was recently incorporated into DICOM, though this has not yet been incorporated into commercial PACS workstations.
Thank you for your interest, @dlrubin
I need to learn more about RadLex and other efforts for standardization in radiology. It is really helpful that you told me the RadLex playbook website and AIM project. I’ll dig into RadLex and the AIM project.
I have two use cases in my mind.
Building artificial intelligence model by using brain CT in patients with suspicious stroke.
Recently, the paradigm for ischemic stroke is shifting from intravenous thrombolysis with tPA into endovascular procedure (mechanical thrombectomy. The ASPECTS (Alberta Stroke Program Early CT Score) is a quantitate score that measures the extent of early ischemic changes. The ASPECTS relies on subtle CT findings and thus requires an experienced radiologist. In Korea, many hospitals usually don’t have experienced radiologist or neurologist in the night. So I want to make help clinicians to calculate ASPECT score by deep learning.
For this purpose, I need to extract only ‘non-contrast’ phase from whole brain CT. By using R-CDM, the same phase of brain CT can be pulled from target cohort (patients with suspicious symptoms for stroke).
And then deep learning model can be developed by using these images (For standardizing the image size, I need three-dimensional resolution, which will be in R-CDM, too). We’ve converted brain CT of 300 patients with suspicious symptom of stroke in our hospital and started to build the model now.
Building predictive model by using clinical and radiology data within PatientLevelPrediction ecosystem.
Recently, I’m trying to develop the model predicting in-hospital mortality by using the deep learning module of PLP packages. On top of the clinical variables, I want add features from ‘chest x-ray’. Like other features generated by FeatureExtraction package, the some features from x-ray can be converted into features by using unsupervised deep learning. And then, features from image can be used for building predictive model with clinical features in PLP ecosystem.
Those two are my future plan. I think I can show the pilot result of first use-case.
I really appreciate your helpful comment, again.
However, until imaging equipment vendors support AIM or the DICOM SR TID 1550 object, this won’t help your use cases, and if R-CDM development is based only on what you can glean from the DICOM header, then there are limits to the info you can capture. I think it will be helpful to access and link info that can be extracted (using NLP) from radiology reports associated with the imaging study to fulfill use case such as yours involving radiology. I have some comments about your two specific use cases:
In order to train a model to predict ASPECTS score, you need a representation of the score (and possibly the imaging features described in the radiology report that led to selection of that score). Is this modeled in R-CDM? Also, in order to recognize DICOM images that are from the “non-contrast phase” series of a brain CT, I presume R-CDM has a model for the value of the SeriesDescription DICOM element (0008,103E) which I believe is where you would determine this? The challenge is that this is a free text field and I’m not aware of any standard terminology for naming the imaging series (the Radlex Playbook/LOINC project so far has only tackled naming imaging study names). I’d be interested to learn more detail about what specifically you did when you say you converted 300 brain CT studies. Finally, in the USA, MRI is generally performed in acute stroke and it might be useful in your deep learning model to work with MRI as well as CT (or separate models for each) if you’re looking for other sites to potentially contribute here.
In terms of adding features from chest x-ray images, are you creating something in R-CDM to represent these features? There’s work going on to standardize description of image features (Image biomarker standardisation initiative), but image features learned from DL models would be challenging to describe/represent in an explicit paradigm. I’m not sure I see how one would describe image features learned from a DL model would be described in R-CDM so they can be linked to clinical features in the PLP ecosystem. Perhaps I’m not understanding the details of this ecosystem.
[Annotation / Report in Radiology]
I know annotation data and ROI are very important, and I need to learn from AIM project. But as you said, I do not have the data containing information about this, now. I suggested the extension model of ‘NOTE’ table for storing radiology report ( https://github.com/OHDSI/CommonDataModel/issues/172 ) , and I hope this proposal to be adopted in OMOP CDM v6.0.
[Question1: imaging for stroke and standardization of DICOM headers]
We leverage information fro DICOM headers, but we cannot totally dependent on it. These informations are not standardized as you said. The solution for identifying the specific phases in radiology images should be developed one by one in each institution for each radiology images. We found out which rule we should use to identify phases in brain CT by browsing DICOM headers.
Again, R-CDM project is in its infancy.
I am really pleased if you can join this research. I can make CNN model for MRI (actually it is much easier to use brain MRI rather than CT, because there is much more open-source code analyzing brain MRI). But I think it would be much more difficult to standardize MRI procedure (The phases are so complicated in brain MRI. But we can start with only T1, T2 and FLAIR for the pilot study.)
[Question 2]
PLP ecosystem requires features in the format of n-dimensional vectors. Actually, I need to figure out how to make feature vectors… It can be done through supervised learning or unsupervised learning. But I do not have concrete idea for this for now.
[R-CDM] Thanks for the link to your draft of this, I see two files but I don’t understand their contents. Is there any documentation describing this?
[Annotation/Report in Radiology]
Since AIM already has a data model for describing the key semantic information in radiology images, I’d encourage that R-CDM describe similar information entities that AIM does, so that interoperability between AIM instances and R-CDM/OMOP will be facilitated. In particular, including AnatomicEntity, AnatomicEntityCharacteristic, ImagingObservation, GeometricShape, ImagingObservationCharacteristic, and Calculation entities would be helpful. Then images that have been annotated using AIM (and soon the AIM/DICOM-SR) compatible tools can interoperate.
[Imaging for stroke and standardization of DICOM headers]
If you are primarily pursuing the stroke use case, it would be good to focus on brain MRI for now. As to standardizing MRI procedure, I agree it’s fine to start with T1, T2 and FLAIR for the pilot study, and put those into the R-CDM model. Then each site would need to map their ad-hoc series names to the equivalent entities in R-CDM.
[Question 2]
For this particular use case, I think you’ll get a lot of signal for prediction by using the radiology report, since that has already been synthesized/summarized by a human. Looking directly at the image data and doing feature extraction from that could be helpful in different use cases, like generating the report (very hard problem), so you might make the problem easier on yourself by using the report text and integrating that with other clinical EMR data as a first pass at this problem.
[Annotation/Report in Radiology]
Yes, we’ll review the AIM and try to make the model compatible with this. Thank you for helpful advice, again.
[Imaging for stroke]
Our job for brain CT is almost done,now. We’ll show the actual use case of this in OHDSI symposium.
Definitely one of the next steps would be standardization of brain MR. But currently, I’m planning to integrate chest x-ray first.
[Question 2]
Thank you for the precious idea. Yes, generating the report is actually one of my dream.
First of all, I’ll predict prognosis of stroke patients with their initial brain CT or predict overall mortality in hospitalized patients with their chest x-ray
Thank to @NEONKID 's effort, we released the ETL module converting DICOM file into Radiology CDM, which can extract required meta-data from DICOM for Radiology CDM.
Thanks for the reply @SCYou. Is there any documentation on R-CDM or how can I get up to speed to understand this model as I think about possibly building on it or pursuing related work?
@dlrubin Thank you for your interest, again.
Sorry that I didn’t prepare the detailed documentation for Radiology-CDM. You can see the abstract about Radiology-CDM for OHDSI symposium 2018, here.
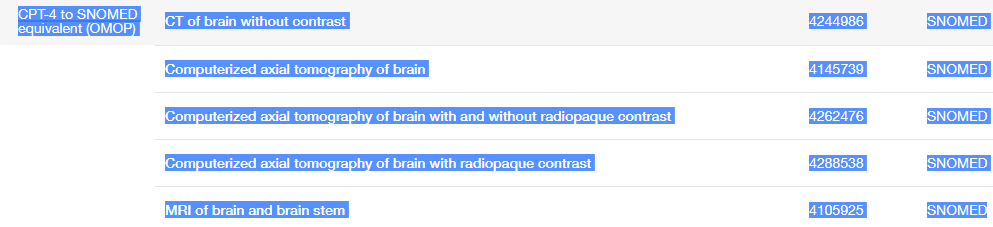
It depends on source data. E.g., if from billing data - we don’t have a good strategy what is the best target terminology. CPT itself is standard concept.
If we have data from more advanced sources (e.g., EHR system) - we may have to think about how these will co-exist with the billing input.
e.g., CT or MRI of the brain performed within 24 hours of arrival to the hospital (STR) concept_id 2106371
concept code 3111F
@Vojtech_Huser
Thank you for the comment. Yes, the adding device_id in R-CDM is definitely one of my goals. I hesitated to add it because ‘device_exposure’ is actually ‘exposure’ table for device, not device itself. So I concerned whether we should add sort of ‘device’ table for ‘device’ itself. Device information is essential for PGHD information (e.g., which wearable device) genetic extension model (e.g., which sequencing device),and radiology information.
Linking with the device_exposure is actually good solution. For brain CT, I want to use ‘45762714’(Full-body CT system) for device_concept_id (http://athena.ohdsi.org/search-terms/terms/45762714), though I’m not sure this is the best term…