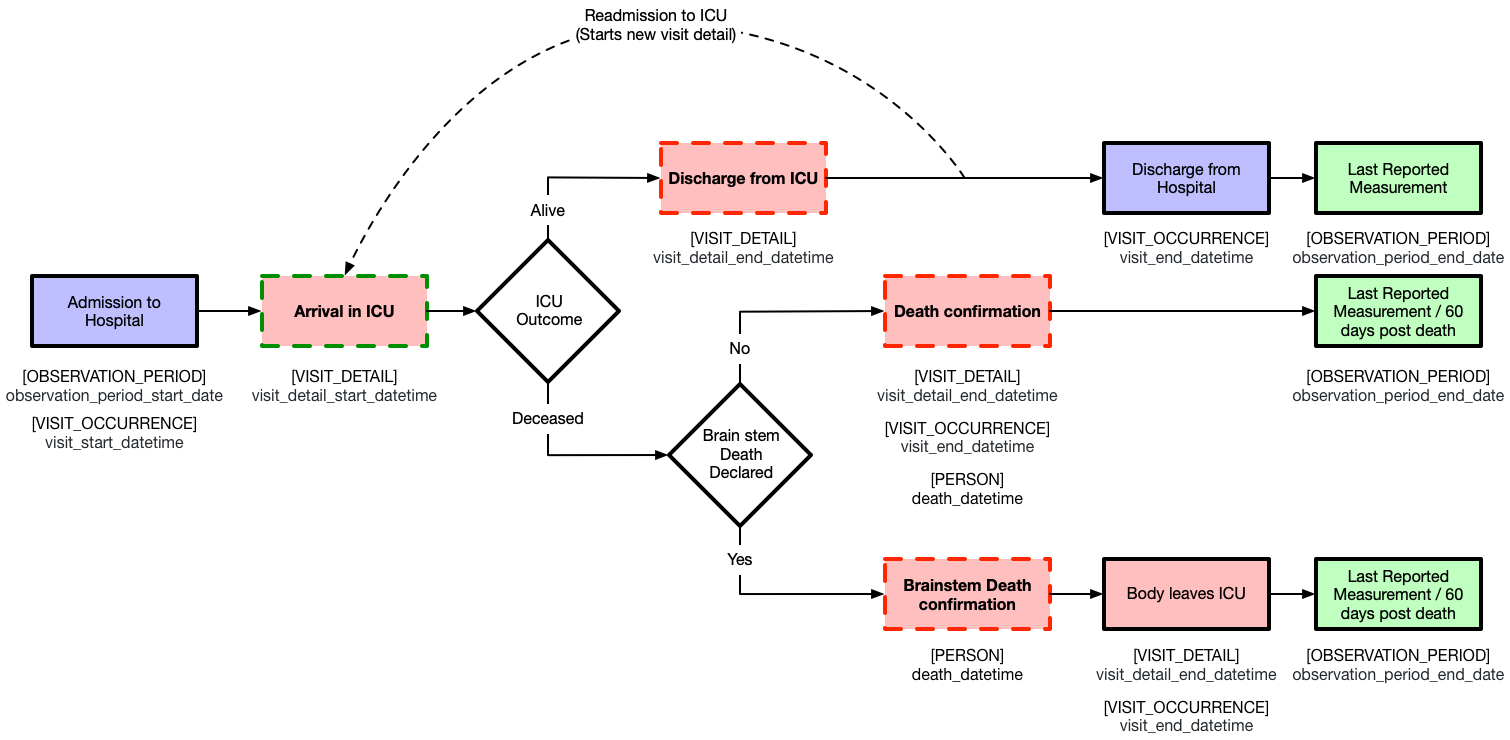
Hi all. I am implementing OHDSI for an intensive care database in the UK. From the ICU perspective, it makes sense to consider each hospital admission, a new “observation period”, with admissions to the ICU a new “visit occurrence”.
There is a logical sequence to the way in which an ICU visit could end. Please see the attached graphic for a detailed explanation. Broadly, after admission, you can either: be discharged alive, or die (of which a small percentage will be via brainstem death). My feeling is that the datetime of death (from whatever cause) should be mapped to VISIT_OCCURRENCE.visit_end_datetime as well as OBSERVATION_PERIOD. observation_period_end_date and PERSON.death_datetime.

I can think of no good analytical reasons to continue to declare the visit or observation period “open” after the confirmation of a death. It would also be hard to pin point a good source of information to determine these times beyond the time of death. However, I can’t see this convention explicitly written anywhere. I would appreciate any advice from the OHDSI community on the correct procedure here?
Many thanks,
Ed
 The complexity and ambiguity of EHR data coupled with the lack of clear conventions increase the complexity of ETL’ing to the OMOP CDM. If you send me your email address, I will add you to the EHR WG invite. It’s an open meeting, but I find it easier to have an invite on my calendar instead of digging through the forums or finding the meeting details on the OHDSI WG meeting
The complexity and ambiguity of EHR data coupled with the lack of clear conventions increase the complexity of ETL’ing to the OMOP CDM. If you send me your email address, I will add you to the EHR WG invite. It’s an open meeting, but I find it easier to have an invite on my calendar instead of digging through the forums or finding the meeting details on the OHDSI WG meeting