Continuing the discussion from Inclusion into vocabulary - Codes for Point of origin, priority of admission and patient discharge status:
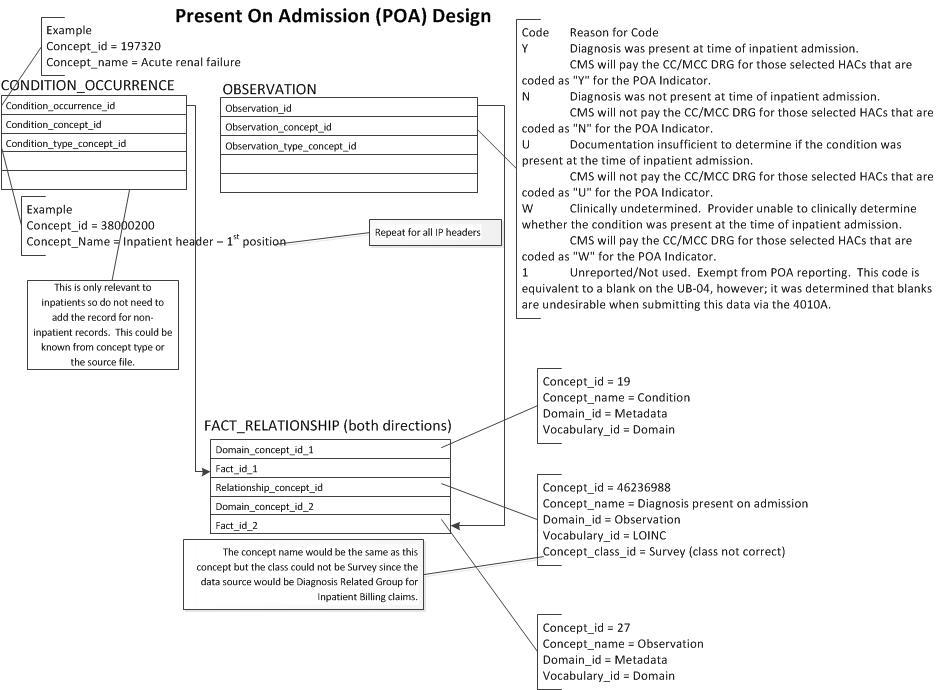
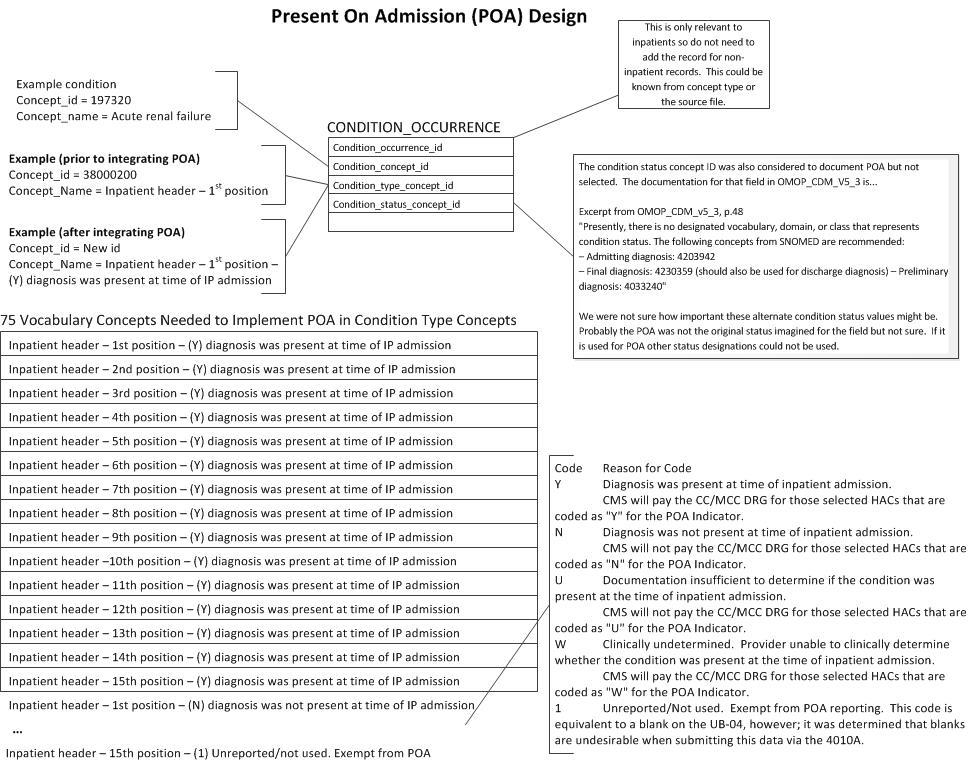
Interested in adding “present on admission” as a concept originating from claims data. There is a similar concept shows in the diagram but the class indicates origination in survey data. We would also want to profile concepts for all the Center for Medicare Services (CMS) profiles for the attribute of whether a condition is present on admission (see diagram and below). In the US, this data is abstracted at discharge for inpatients and is high quality as it is in part a basis for reimbursement as well as a flag for hospital acquired conditions. I am not sure if this is part of transitions of care.
Code Reason for Code
Y Diagnosis was present at time of inpatient admission.
CMS will pay the CC/MCC DRG for those selected HACs that are coded as “Y” for the POA Indicator.
N Diagnosis was not present at time of inpatient admission.
CMS will not pay the CC/MCC DRG for those selected HACs that are coded as “N” for the POA Indicator.
U Documentation insufficient to determine if the condition was present at the time of inpatient admission.
CMS will not pay the CC/MCC DRG for those selected HACs that are coded as “U” for the POA Indicator.
W Clinically undetermined. Provider unable to clinically determine whether the condition was present at the time of inpatient admission.
CMS will pay the CC/MCC DRG for those selected HACs that are coded as “W” for the POA Indicator.
1 Unreported/Not used. Exempt from POA reporting. This code is equivalent to a blank on the UB-04, however; it was determined that blanks are undesirable when submitting this data via the 4010A.